



Abstract
Purpose: The objective of this pilot study was to demonstrate the number of patients at increased risk for type 2 diabetes development using a validated survey; and to assess the rate of compliance for A1c screening in an educational dental hygiene setting.
Methods: This was a descriptive study using a purposive sample of patients in an academic dental hygiene clinic, who were 18 years or older, not diagnosed with prediabetes or type 2 diabetes. Utilizing the American Diabetes Association adopted diabetes risk survey, patients determined to be at increased risk for type 2 diabetes were offered the opportunity for further assessment by having their A1c tested using a point of care instrument. Patients demonstrating an increased risk for prediabetes or type 2 diabetes, with either the survey or the point of care instrument, were referred to their primary physician for further evaluation.
Results: A total 179 of the 422 solicited patients agreed to participate in the American Diabetes Association adopted diabetes risk survey. According to the survey guidelines, 77 participants were considered increased risk for type 2 diabetes for an at-risk prevalence of 48% (95% Confidence Interval (CI): 40 to 56%). The at-risk participants were then asked to have an A1c test of which 45 agreed (compliance rate 58%, 95% CI: 47 to 70%). Using American Diabetes Association A1c parameters, 60.98% (n=25) indicated a prediabetes (5.7 to 6.4%) range, and 4.88% (n=2) indicated a diabetes (≥6.5%) range.
Conclusion: Utilizing the American Diabetes Association adopted diabetes risk survey in any dental setting could provide patients with invaluable health information, and potentially improve overall health outcomes.
Introduction
A systematic analysis of the global prevalence of type 2 diabetes found the number of adults with diabetes doubled over a 30 year period, increasing from 153 million in 1980 to 347 million in 2008.1 The World Health Organization (WHO) estimates diabetes will be the seventh leading cause of death in 2030.2 In 2012, there was an estimated 1.7 million new cases of diagnosed diabetes among U.S. adults 20 years and older.3 Between 2009 to 2012, utilizing fasting glucose or A1c levels, 37% or 86 million Americans aged 20 years or older had prediabetes, 51% of those were aged 65 years or older.3 In addition, the Centers for Disease Control most up-to-date scientific data estimates 8.1 million individuals or 27.8% of the U.S. population have undiagnosed diabetes.3
The estimated cost associated with diagnosed and undiagnosed diabetes in 2012, was over $322 billion, including $244 billion in medical costs and $78 billion in decreased productivity.4 This cost translates to an economic burden of over a $1,000 for every American.4
Diabetes can lead to more serious health complications like blindness, kidney damage, cardiovascular disease and lower limb amputations.3 The prevalence and effect of diabetes are compelling enough to stress the need for early diagnosis and treatment. Early diagnosis can alleviate many of the complications associated with diabetes and prevent disease progression.3
Identification of Prediabetes and Diabetes
Diabetes can be diagnosed based on A1c or fasting plasma glucose level, the fasting plasma glucose or the 2-h plasma glucose value subsequent to a 75-g oral glucose tolerance test.5,6 There is an increased risk of developing type 2 diabetes based on older age, obesity and lack of physical exercise in individuals with hypertension and, in particular, racial/ethnic subgroups (African American, American Indian, Hispanic/Latino and Asian American).7 Most often there is a lengthy period without symptoms prior to the diagnosis of type 2 diabetes.7
In Healthy People 2020, the U.S. Department of Health and Human Services includes screening for type 2 diabetes as one of the top measures to be implemented in the health care system.8 As part of the U.S. health care system, the dental profession can play an integral role with implementation.
Diabetes and Periodontal Disease
Diabetes and periodontal disease are 2 chronic diseases considered to be biologically linked.9,10 Periodontal disease is a chronic inflammatory disease of the supporting tissues of the teeth and the primary cause of tooth loss for older adults.11,12 It is estimated 47% of U.S. adults 30 years and older have periodontitis, the destructive form of periodontal disease.13 Evidence over the last 15 to 20 years supports an association between periodontal inflammation and glycemic control among individuals, with or without diabetes, and the complications associated with diabetes.10 There is a well-established understanding that periodontal outcomes are affected by hyperglycemia.10 Additionally, evidence increasingly supports a likely association between systemic inflammation and oral microbial agents in circulation.10
The Dental Office as a Gateway to Medical Screenings
Prediabetes and diabetes are 2 conditions where screening and early recognition would be beneficial to prevent public health burdens.7 The increasing public health burden of diabetes requires a collaborative approach among health care providers, in order to identify and manage its complications.10 A survey of 1945 practicing dentists in the U.S. suggested dentists thought medical screenings were important and were willing to incorporate screenings for medical conditions in the dental office, including diabetes mellitus at a 76.8% rate of agreement.14
In 2013, 61.7% of adults between the ages of 18 and 64 had a visit with their dental provider.15 For patients who are not utilizing health care services and visit a dental office for emergency situations, health care screenings may be done at these visits.10
A prospective study was conducted within Columbia University College of Dental Medicine Triage Clinic to explore the development and evaluate the performance of a selective approach to identify undiagnosed prediabetes and diabetes in a dental setting.16 Participants (n=601) were selected based on one self-reported risk factor for diabetes and subsequently evaluated utilizing a periodontal exam and an A1c point of care instrument.16 The study findings confirmed the approach was effective in identifying individuals (n=182) with potential undiagnosed diabetes and prediabetes and referring them to a physician for evaluation.16 The researchers conclude their model of identification should be further explored by dental professionals and validated in diverse dental populations.16
In a study by Genco et al, 11 general dentistry and periodontal specialty practices including a community dental clinic, utilized the American Diabetes Association Risk Test and a point of care instrument to measure hemoglobin A1c among 1,022 participants.17 They identified individuals (n=416) with potential diabetes or prediabetes and referred them to a physician for further evaluation.17 The study demonstrated dental screening feasibility for diabetes and prediabetes, as well as acceptance among dental staff, patients and their physicians.17 Although the Genco et al study had notable findings, due to various barriers including lack of insurance coverage for screenings in a dental setting, and patient's lack of compliance for follow-up after screening in private dental practices, the authors were hesitant to recommend diabetes screenings in traditional dental settings.17
An 8 item survey of randomly selected patients from a New Jersey Dental School and several private practice clinics (n=470) was conducted regarding patient attitudes toward chairside medical screening in a dental setting.18 The responses of the majority of the participants were favorable towards having a dentist perform screening for heart disease, high blood pressure, diabetes, human immunodeficiency virus infections and hepatitis infection.18
A cross-sectional study conducted by Creanor et al utilized a 1-page questionnaire among patients within 2 primary care dental clinics and 16 general practices in South-West England.19 The survey was designed to determine attitudes toward chairside medical screenings, including diabetes, among patients attending appointments at primary care dental clinics and general dental practices.19 A total of 626 surveys were completed from 18 sites at an 87% rate of agreement for the importance of dentists screening for medical conditions.19
As part of The Dental Practice-Based Research Network, a study in 28 community dental practices recruited 498 patients to test the feasibility of screening for abnormal random blood glucose levels using glucometers and finger-stick testing.20 Among the participants, greater than 80% liked the idea and 62% would recommend their dentist to others, if blood glucose testing was available.20
The purpose of this pilot study was to implement the American Diabetes Association diabetes risk test to identify patients at risk for undiagnosed type 2 diabetes in an educational dental hygiene setting and to determine the rate of compliance and results when a point-of-care A1c screening was recommended.
Methods and Materials
This descriptive study consisted of a purposive sample of patients at an academic dental hygiene clinic. Permission to utilize the validated diabetes risk test was granted by the American Diabetes Association. The American Diabetes Association diabetes risk test questionnaire included age, sex, history of gestational diabetes, family history of diabetes, physical activity and weight. A score of 5 or higher on the diabetes risk test indicated an increased risk for developing type 2 diabetes. In addition to the 7 questions, 2 yes/no response questions were included. The first question inquired of a previous diagnosis of high blood sugar, borderline diabetes, prediabetes or diabetes type 1 or 2. The second question was presented at the end of the American Diabetes Association risk test, and inquired of participant's willingness to have a finger stick to measure 2 to 3 month average blood glucose, if their risk test score indicated increased risk for type 2 diabetes (≥5). Considering health literacy levels, the term A1c was omitted from the second question, and replaced with blood sugar. Two principal investigators and 1 clinic staff member, all registered dental hygienists, administered the study informed consent forms, the A1c tests and completed follow-up referral letters. Dental hygiene students administered a National Cash Register carbonless 2-page paper version of the American Diabetes Association diabetes risk test.
Eligibility criteria for the study included all patients who presented to the clinic who were 18 years or older not previously diagnosed with prediabetes or diabetes. Exclusion criteria included participants with a preexisting diagnosis of high blood sugar, borderline diabetes, prediabetes, or diabetes mellitus type 1 or type 2. The university's institutional review board ensured the protection of the subjects engaged in this study.
During appointment check-in, study personnel provided patients an implied consent form which explained the study, and participants in agreement self-completed the American Diabetes Association diabetes risk test. Once the risk test was completed, dental hygiene students identified participants determined to be at increased risk for diabetes and alerted study personnel. Participants who scored a 5 or greater and indicated yes to having their average blood glucose measured had their A1c tested via a point of care instrument, the DCA Vantage™. The DCA Vantage™ was found to meet the acceptance criteria of the National Glycohemoglobin Standardization Program certification criteria of A1c instruments, making it equivalent to laboratory-based methods.21,22 Participants with A1c indicative of prediabetes or diabetes based on the American Diabetes Association guidelines, 5.7% or greater, referred to their primary physician for further assessment.5 Additionally, a copy of the completed American Diabetes Association risk test, the results of the A1c test, and an accompanying letter explaining patient's risk were mailed to the physician of record.
The questionnaire responses were entered into electronic format via Microsoft Excel. A quality assessment was undertaken by which a random sample of written surveys were audited for data-entry error. The analysis included descriptive statistics using frequency percentiles, with Wald and Exact Binomial 95% CI calculated for selected variables. Associations between select variables were assessed via contingency tables and Fisher's Exact Test. The main analysis used data from all patients who participated in the survey who did not have known pre-existing diabetes conditions (n=159). To assess robustness of study results to missing data, sensitivity analyses were performed via full case analysis (n=145) and mean imputation for missing values (n=159). All statistical analyses were performed in STATA® statistics/data analysis software version 11.2.
Results
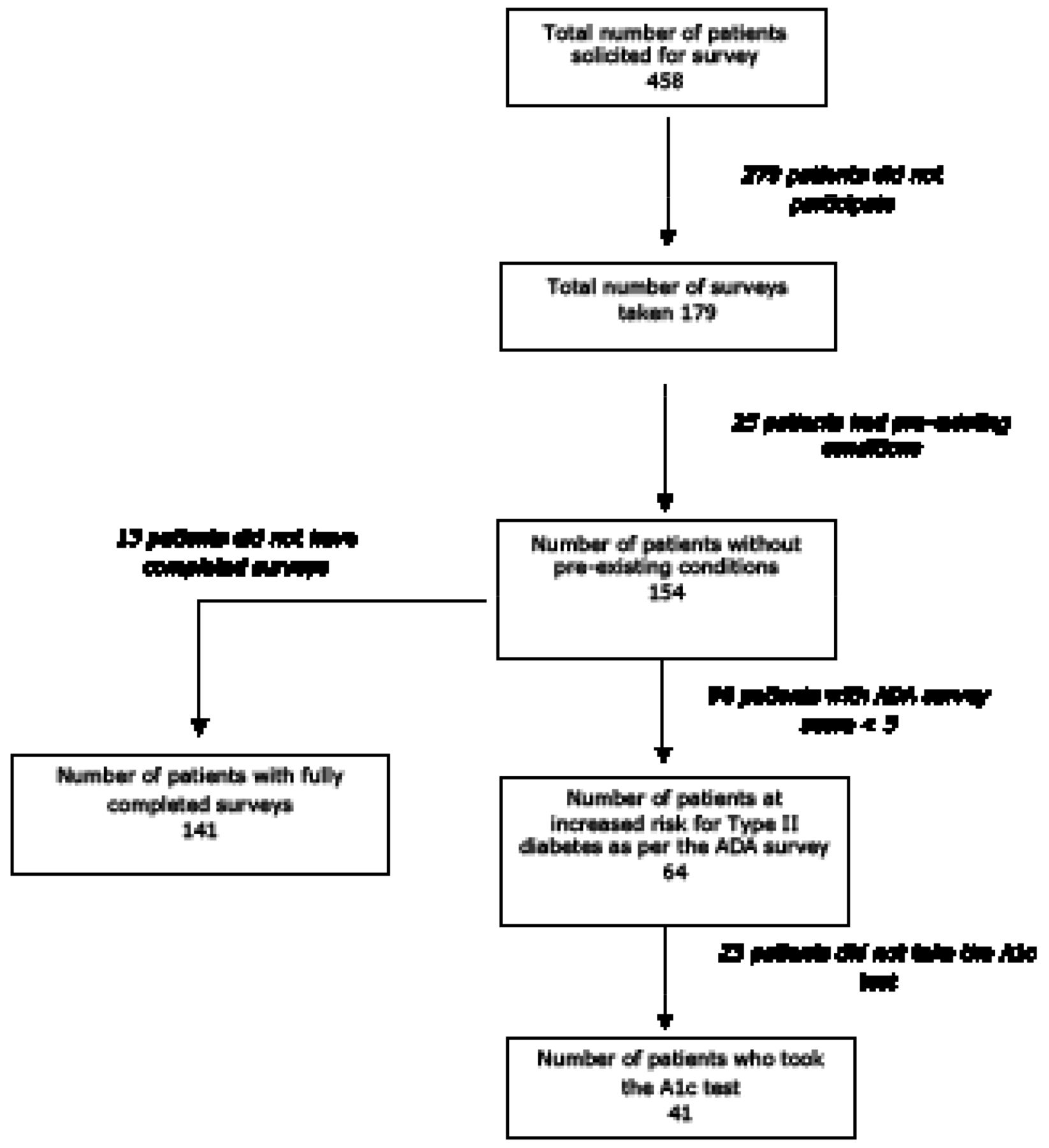
The study profile of solicited study patients is shown in Figure 1. A total of 179 of 458 solicited patients agreed to participate in the study (compliance rate 39%, Binomial 95% CI: 35 to 44%), with 25 of the 179 study participants reported known pre-existing prediabetes or diabetes conditions and did not meet study criteria. As per the American Diabetes Association diabetes risk test, 64 of the 154 participants without pre-existing conditions included in the analysis were at increased risk for type 2 diabetes with an at-risk prevalence of 42% (Binomial 95% CI: 34 to 50%). Of the 64 participants who were determined at risk, 36 reported they would take the A1c, 5 reported they would not, and 23 did not report an answer. Once the 64 at-risk patients were informed of their risk score as per the American Diabetes Association diabetes risk test by research personnel, 41 patients took the A1c test offered. (Compliance rate 64%, Binomial 95% CI: 51 to 76%).
Table I shows descriptive statistics of the study population included in the analysis (n=154). The majority of patients were female (66%), 50 years of age or older (65%), reported no physical activity (79%), did not have a previous high blood pressure diagnosis (68%) and did not have a direct family member with diabetes (66%). Associations between demographics and response to take the A1c are shown in Figure 1. No statistically significant associations were found between demographic variables and patient responses to take the A1c test. Of the 41 patients who did receive the A1c test, the mean A1c was 5.82% (95% CI 5.70 to 5.96%), as shown in Table II. As per the American Diabetes Association parameters, the majority of patients (61%) scored an A1c between 5.7% and 6.5% indicating increased risk for diabetes.5

Associations between Demographics and Compliance for A1c Screening
Discussion
Among the undiagnosed patients who participated in the American Diabetes Association risk test, 42% were found to be at increased risk for diabetes and were then referred to their physician for further evaluation. Even without A1c testing, administering the American Diabetes Association risk test was found to be a beneficial health promotion tool for identifying patients at risk for developing diabetes.
There was a 64% rate of agreement among the high-risk group to have their A1c tested. The administration of the American Diabetes Association diabetes risk test created an opportunity for dialogue between the patient and the oral health care provider. Moreover, the utilization of the diabetes risk test in a dental setting may provide incentive for follow-up with a physician. Based on the point of care instrument, the majority (61%) had an A1c in the prediabetes or diabetes range. Although a point of care A1c assay is not recommended for a diagnosis of prediabetes or diabetes, an A1c test should be done in a laboratory using a method meeting National Glycohemoglobin Standardization Program and Diabetes Control and Complications Trial certification and standards; it may serve as a convenient screening tool and improve patient compliance for physician follow-up.7 Patients were provided with a written referral and the principal investigators sent a copy of the American Diabetes Association diabetes risk test along with a letter to the physician of record for further patient evaluation.
Demographic Characteristics of Study Population
A1c Test Results
The rate of participation among patients who took the American Diabetes Association diabetes risk test may be explained by the length of time it takes a patient to receive preventative dental hygiene services in an educational setting. Relying on the front office and/or dental hygiene students to administer the American Diabetes Association diabetes risk test at the start of the patient appointment was not a reliable method of administration. Incorporating the American Diabetes Association diabetes risk test along with other risk assessments conducted during the dental hygiene process of care may improve the rate of compliance and reinforce the association between diabetes and periodontitis.
National data indicate the incidence and prevalence of prediabetes and diabetes is on the rise.1 Type 2 diabetes is a manageable disease with early diagnosis. The majority of adult patients have an annual visit with a dental provider, and implementation of the American Diabetes Association diabetes risk test can help to identify patients at increased risk for diabetes. The tool could be utilized in any dental setting to provide patients with important health information, potentially improving health promotion and disease prevention.3 Large scale clinical trials need to be conducted to assess feasibility, acceptance and cost-effectiveness of screening in a dental as comparted to a medical setting.
Health screenings are more cost-effective than the treatment of disease and could potentially ease the economic burden of diabetes care.4 Additionally, implementation of a health screening tool within a dental setting could provide an opportunity to increase collaboration among dental and medical providers.
A study limitation included lack of patient-physician follow up to determine confirmation of diagnosis. Additionally, the authors recognize this was a relatively small sample population in one location and therefore not generalizable.
Conclusion
Utilization of the American Diabetes Association risk test assisted in identifying type 2 diabetes at risk patients, and provided an opportunity to discuss diabetes in a dental setting. Moreover, utilization of the diabetes risk test in a dental or dental hygiene setting may provide incentive for follow-up with a physician. As healthcare providers, dental professionals have a responsibility to raise diabetes awareness. Future research regarding diabetes assessment in a dental setting must be conducted to better understand the value of screening in a dental setting, and to investigate if this form of screening leads to improved diagnosis and management of diabetes.
Acknowledgments
The authors thank MCPHS University for the funding of this project through a faculty development grant. Special thanks to Lory Libby, RDH, MS, for her clinical assistance.
Footnotes
Lori J. Giblin, RDH, MS, is an Assistant Professor, Forsyth School of Dental Hygiene, MCPHS University. Lori Rainchuso RDH, MS, is an Associate Professor and Graduate Program Director, Forsyth School of Dental Hygiene, MCPHS University. Andrew Rothman, MS, EIT, is a doctoral candidate at Harvard School of Public Health and Adjunct Faculty at Forsyth School of Dental Hygiene, MCPHS University.
This study supports the NDHRA priority area, Health Promotion/Disease Prevention: Validate and test assessment instruments/strategies/mechanisms that increase health promotion and disease prevention among diverse populations.
- Copyright © 2016 The American Dental Hygienists’ Association





{kind=link}