



Abstract
Purpose: The objective of this study was to investigate knowledge and perceptions of executive directors of long-term care facilities in a large western state regarding oral health of residents, barriers to the provision of optimal oral health care and the collaborative practice role for dental hygienists.
Methods: A descriptive, exploratory online survey research design was utilized. A purposive sample of executive directors of long-term care facilities in a large western state certified for Medicare/Medicaid reimbursement was used. An online survey was developed to investigate perceptions and knowledge regarding oral health of long-term care residents, protocol for provision of, and barriers to optimal oral health care, and support for employment of dental hygienists in long-term care facilities. Statistics used for data analysis included frequency distributions, Spearman's rho correlation coefficient and the Mann-Whitney test.
Results: Executive directors in long-term care facilities included in the study perceived oral health as an important aspect of general health; however, a knowledge deficit was identified related to oral disease as an exacerbating factor to systemic disease. Financial concerns and low interest among residents/families were identified as major barriers to accessing care. Executive directors supported interprofessional practice of nurses working with dental hygienists to optimize oral health care of residents. No significant associations were found between demographics and facility characteristics.
Conclusion: Awareness of the knowledge and perceptions of executive directors providing leadership in these facilities can provide avenues to creating needed change, which can foster improvement in the oral and overall health status of long-term care residents. Support for interprofessional work of nurses and dental hygienists can open a door for innovative practice that optimizes oral health care of long-term care facility residents through the application of shared expertise.
Introduction
By the year 2040, approximately 25% of the U.S. population will be over age 65.1 People are living longer and retaining more of their natural dentition. Retention of the natural dentition predisposes older adults to dental caries and periodontal disease. Untreated dental and periodontal diseases may intensify health problems in an already medically complex population. Oral health has been identified as a key factor in general health and systemic disease in long-term care populations.2-5 Oral infection contributes to poor outcomes in persons with metabolic, cardiac, cerebrovascular and pulmonary disorders, and all are more prevalent conditions in older adults.2-5
The dental and oral health care needs of aging adults residing in long-term care facilities are not being adequately met due to several key factors:1-6
Lack of knowledge of the importance of oral health care on the part of residents, their families, and the staff
Difficulties faced by residents in performing self-care due to physical limitations
Dementia and/or behavioral problems, making it difficult for patients and staff to perform needed care
Ageism prejudices evident among staff and families
Severely limited reimbursement for professional dental services as well as inadequate financial standing among residents
Poor oral health in elderly adults upon admission to a facility
Aging long–term care residents are more susceptible to clinically significant oral health problems including fungal, viral and bacterial infections, severe dry mouth (and other drug side effects), and/or loss of function from missing/diseased teeth and ill-fitting oral appliances. Oral infections may lead to more severe systemic and life-threatening infections such as pneumonia, cerebral abscess, bacterial endocarditis, osteomyelitis and septicemia.4,5 Abundant evidence exists denoting poor oral health of long-term care residents and barriers to provision of oral care, yet there is no consensus as how best to address these problems within or outside the dental profession.6-9
Legislation has been introduced in Utah to create a strategy which would allow dental hygienists to better address the oral health needs of underserved populations, including long-term care residents. During the 2012 general session of the Utah State Legislature, the state in which this study was completed, H.B. 125: Access to Dental Health Care, was passed. This legislation established a plan to pilot dental health care payment and delivery reform models and to evaluate cost. The program extends Medicaid coverage to provide dental care for some adults with limited access to dentistry, and residents of long-term care facilities comprised a major section of the study sample. Lines 62 to 64 of the bill state, “The pilot program shall establish compensation models for dentists and dental hygienists that: increase access to quality, cost effective dental care…”10 While hiring a dental hygienist may require legislative changes, depending on the state, having a dental hygienist on the team can contribute to an improved level of care or provide oversight to nursing assistants in developing oral care plans tailored for each resident.11-13
Knowledge and perceptions of executive directors with respect to oral health of long-term care residents have not been well-studied and documented. A 2005 survey of executive directors of all long-term care facilities in Ohio investigated how the oral health of residents was perceived. Knowledge, interest, value and priority assigned to the oral health of those residing in facilities were assessed. All responding executive directors valued oral health and agreed that it was an integral part of general health. A vast majority expressed a high level of importance for oral care, yet half considered oral health a lower priority than general medical care. A total of 53% rated their residents' oral health as fair or poor but were still satisfied with the oral care provided at their facilities, illustrating the critical nature of executive directors' attitudes toward oral health.14 In a study of long-term care administrators completed in Michigan, executive directors perceived a lack of willingness on the part of dentists to provide oral health care to residents in the dental office or facility, creating a major barrier to oral health provision.15 Ekelund evaluated oral health training programs and reported that only 20% of long-term care executive directors considered oral care more important than hairdressing. That perception underscores the importance of executive directors' attitudes toward oral health if improvement for residents is to be achieved.16
The Targeting Revolutionary Elder Care Solutions (TRECS) Institute, a non-profit organization dedicated to the improvement of health care for residents in the long-term care industry, undertook a study designed to identify methods of assuring better dental and oral care services for residents in Florida nursing homes. In the final report, the TRECS Institute research team made 2 recommendations directly relating to findings from this study. First, it was suggested that development of a “commercial dental insurance program specifically designed for nursing home residents should be tested as a realistic approach to improving dental care services by increasing reimbursement for dental professionals thereby eliminating the access problem that dominates the industry today.”17 A second proposal generated from the study supported that the scope of practice for dental hygienists be expanded by allowing collaborative relationships with dentists similar to the relationship nurse practitioners share with their collaborating physicians in many states.17
Executive directors of long-term care facilities are in prime positions to provide direction for oral health care professionals and lawmakers to positively impact the oral health of this increasing portion of the population. Their knowledge, perceptions, and roles concerning the oral health of long-term care residents may hold implications for the role dental hygienists can play in improving the general and oral health of the residents. Executive directors are key stakeholders for engaging interprofessional health care teams to meet the oral health needs of frail aging residents of long-term care who are dependent on others for their daily care. The executive director is in a position to initiate innovative changes in oral health policies and management of health care personnel that can improve the oral care and health status of residents.
Conceptual Framework
The key concept in this study is role definition, and how this can influence action to improve the health care of older adults in long-term care settings. An individual's knowledge and perceptions define how one's role is realized, and role definition can influence action.18 The executive director of a long-term care facility has a crucial responsibility in overseeing provision of care. Although the nursing professional provides most direct patient care, in assistance with care providers from other disciplines, the executive director is responsible for leadership and quality of care within this health care system. All caregivers involved in direct service provision are influenced by the role of the executive director whose leadership provides guidance in care coordination and delivery. Ultimately, executive directors have a vital role in implementing meaningful reforms to improve care for long-term care residents.18
Given that little data exists related to executive directors' perceptions of oral health in long-term care facilities, this study was designed to answer the following research questions:
What are the knowledge levels and perceptions of executive directors regarding the oral health of residents?
What are the current methods of oral health care delivery and barriers to provision of oral health care in the facilities in which the executive director has a primary leadership role?
What level of support do executive directors have for legislative initiatives to change supervision laws regulating the practice of dental hygiene in long-term care settings?
What level of support do executive directors have for employment of dental hygienists in long-term care facilities?
Methods and Materials
Sample
Study participants included a purposive sample of executive directors employed in long-term care facilities that were certified for Medicare/Medicaid reimbursement in the state of Utah. Deliverable email contact information was obtained for executive directors employed in 80 of the 100 certified long-term care facilities in Utah. The web-based, self-administered survey was e-mailed to executive directors through the utilization of a SurveyMonkey® questionnaire. Executive directors were sent an email to invite participation and obtain informed consent, followed by 2 reminders at 7 day intervals.
Survey Design
The Institutional Review Board of Idaho State University approved this study. A descriptive, exploratory design was utilized. A 29-item survey was developed by the primary investigator to address 3 main themes:
Knowledge and perceptions of executive directors regarding the oral health of facility residents
Oral health care delivery methods for residents
Level of support for employment of a dental hygienist and legislative initiatives to extend the scope of practice for dental hygienists in long-term care facilities
Executive Director Demographics and Facility Characteristics
Statistical Analysis
Upon completion of data collection, results were analyzed using SPSSTM 16.0 software. Nonparametric tests were used including Spearman's rho correlation coefficient and Mann-Whitney Test statistics to calculate measures of association. Statistical significance was set at p<0.05.
Results
Of the 80 executive directors, 38 responded to the email survey, resulting in a 48% response rate. Participating executive directors' demographics and facility characteristics are illustrated in Table I. As can be seen from this table, a majority of respondents were male, with age distribution appearing to be equal between 30 to 39 and 50 to 59 years of age. A majority of the facilities had 51 to 100 beds. Most facilities were located in urban areas and were proprietary in nature. No significant associations were found between demographics and facility characteristics and other responses.
Executive Directors' Oral Health Knowledge and Perceptions
A total of 73% of executive directors (n=38) reported having a written protocol for oral health procedures to be completed by nursing staff, frequency for provision of oral care, procedures for referral to a dentist and documentation requirements. Fifty-one percent indicated no protocol for oral health in-service training for nursing staff. Most facilities do not have a regular protocol for presenting oral health in-service training for nursing staff. Training that is provided is presented by nursing staff themselves. Of the facilities that provide training, the majority include demonstrations of proper techniques for providing daily oral health care, explanations regarding the effect of oral health on physical health and staff assignments for the provision of and barriers to oral care. Fewer include instruction on how to recognize oral infection or caries. Within these facilities, most daily oral care is performed by the residents themselves or by certified nursing assistants. Only 63% of responding executive directors reported that a dentist is affiliated with the facility. Most of these dentists provide in-house screening examinations. Half provide in-house emergency treatment. Almost no facilities have on-site dental equipment. Only 27% reported that a dentist comes on-site at least monthly.
Barriers Limiting Access to Oral Health Care
Interest and Support for Dental Hygiene Services
A majority of the executive directors perceived residents' oral health as good and most considered oral health an important aspect of general health (Table II). Fifty percent of respondents agreed that dental care is as important as general nursing care.
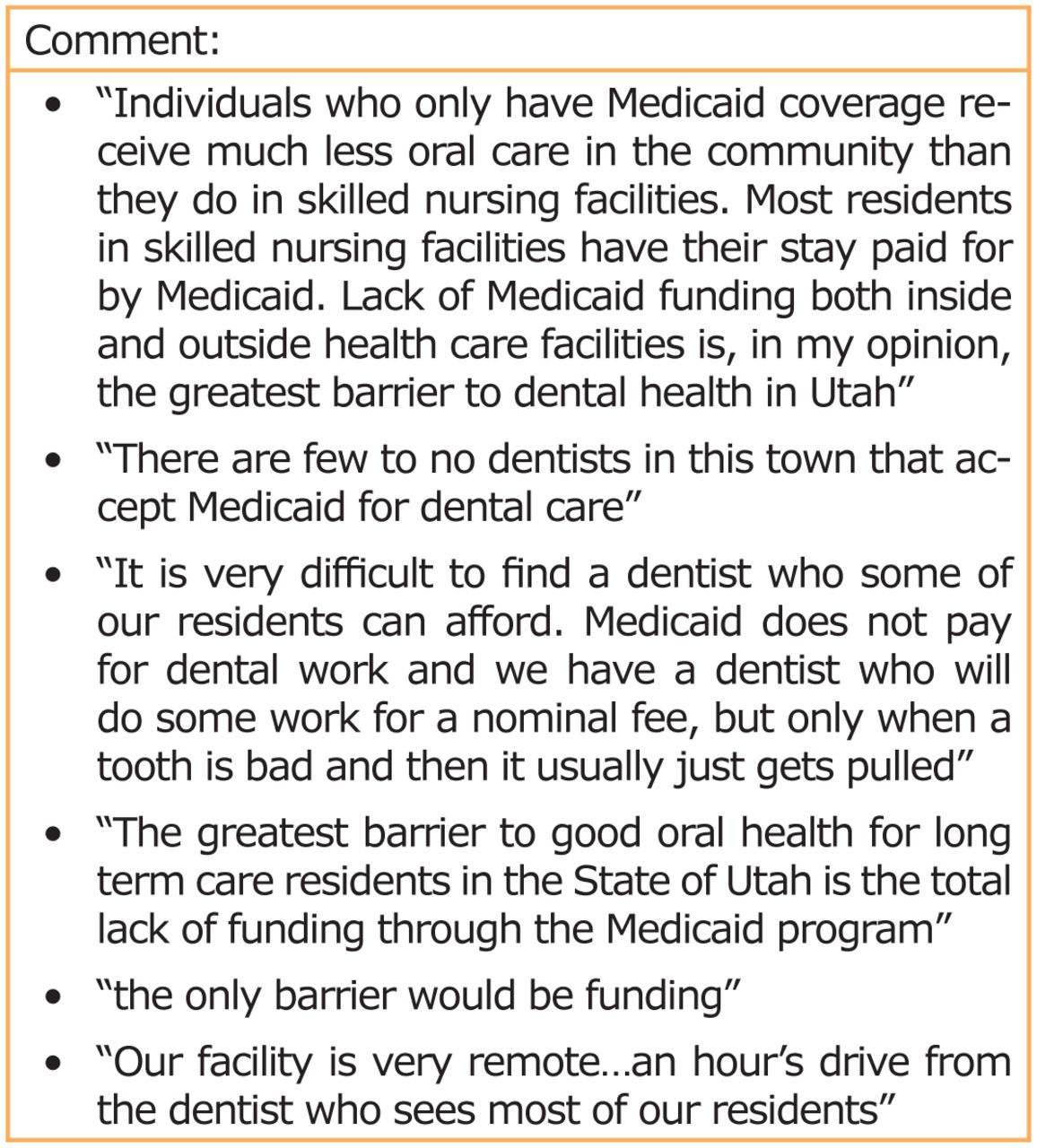
Lower levels of knowledge were evident when executive directors were asked how strongly they felt medical conditions may be exacerbated by oral infection. A significant number indicated that financial concerns were a major barrier limiting access to oral health care by long-term care facility residents (Table III). Level of dementia was another major limiting factor while transportation was deemed the least limiting barrier. Comments from the open-ended questions reflected this concern as well (Figure 1).
Respondents indicated a high level of support for the inclusion of a dental hygienist professional in the care of long-term care residents. Forty percent supported employment of dental hygienists in the long-term care setting. Results indicated interest in having dental hygienists provide an extension of oral care delivery in this setting. Additionally, executive directors indicated a “somewhat” to “extreme” interest level in a dental hygienist providing screening, training, education and preventive care to residents of the long-term care facility (Table IV).
Discussion
The inclusion of a dental professional in the care of the aging adult in the long-term care facility allows for interprofessional collaboration that may improve the health status of a growing and vulnerable population.11-13,19,20 Protocols and support for oral health in-service training involving the dental hygienist can facilitate opportunities for knowledge building and shared expertise, with a goal of improving the oral health and overall health status of residents.11,12 Research has shown that implementation of effective oral health interventions and inclusion of dental hygienists as part of a collaborative healthcare team results in decreased costs and improved health status in older adults.12,13,19,20

Executive Directors' Comments
Executive directors participating in this study were slightly less interested in employing dental hygienists for provision of these services than they were in having dental hygienists provide oral health training to staff. This small difference may be attributed to a perceived inability to hire and reimburse their professional staff in a manner that makes working with long-term care facility residents an economically sound business model.21 Executive directors realized there are barriers to accessing dental care, and funding was by far the most limiting factor in providing oral health care for residents. Unfortunately, payment for oral health care is primarily the responsibility of individual residents, and as a result, they may forego regular dental visits. This decision to “do without” can have serious consequences, and can lead to increased risks for oral infection and associated systemic disease.21-23
An interprofessional perspective where both nursing and dental hygiene professionals contribute expertise could be used to co-develop individualized prevention and treatment care plans for long-term care residents.24 This innovative idea is supported by the finding that Utah executive directors perceive a benefit to having dental hygienists train caregivers within their facilities as well as provide a variety of preventive oral services. Hygienists are well-suited to offer preventive services, educate staff and residents, act as liaisons between dentists and long-term care facility personnel, and serve as champions of oral health for residents. Moreover, by the nature of their educational preparation, dental hygienists are considered to be experts in the areas of preventive oral care, oral health promotion and knowledge of the oral-systemic link.12,25,26
While providing insight and useful baseline data, there were several limitations of this study. The research does not reflect a representative sample of executive directors, as only the executive directors of long-term care facilities in Utah were included to support this initial, exploratory research. The survey items consisted of close-ended questions that may not exactly represent participants' actual perceptions, knowledge or behaviors. Furthermore, this method was descriptive and cannot offer insight into cause-and-effect relationships.
Conclusion
This study provides preliminary evidence that executive directors are open to innovative changes to improve oral health for residents. There may be an opportunity for improving the health of long-term care residents through collaboration with dental hygienists and other health care providers in these settings. Further studies should build on these initial findings to examine the cost-benefit ratio for employment of dental hygienists in long-term care facilities, as well as explore outcomes in oral health status of long-term care residents who receive direct and indirect care from a dental hygienist, and test the recommendations presented by the TRECS Institute.
Footnotes
-
Patricia Wintch, RDH, BSDH, MSDH, is a dental hygiene educator at Dixie State University in St. George. Tara Johnson, RDH, PhD, is an Assistant Professor in Dental Hygiene at Idaho State University. JoAnn R. Gurenlian, RDH, PhD, is Professor and Graduate Program Director of the Department of Dental Hygiene at Idaho State. Karen Neill, PhD, RN, SANE-A, is an Associate Director for Graduate Studies and Professor in Nursing at Idaho State University School of Nursing.
-
This study supports the NDHRA priority area, Health Services Research: Identify how public policies impact the delivery, utilization, and access to oral health care services.
- Copyright © 2014 The American Dental Hygienists’ Association





{kind=link}