



Abstract
Purpose: The purpose of the project was to identify the oral health status and needs of the older adult population ≥60 years old in Illinois for policy decisions and to help identify possible need for oral health interventions. No baseline data has previously been collected on this population in Illinois.
Methods: A public/private collaboration was formed, which included the Illinois Department of Public Health, the IFLOSS Coalition and dental and dental hygiene schools in Illinois. The screening tool was developed based on methods outlined by Association of State and Territorial Dental Directors for Basic Screening Surveys. Questionnaires and in-mouth screenings were conducted at selected sites statewide. Data was collected by dental and dental hygiene students and faculty at onsite clinics and community outreach sites.
Results: A total of 437 seniors were screened statewide. Of this population, 81% had no dental insurance, 13% were edentulous and 58% claimed to have had a dental visit in the last year.A total of 26% rated their oral health as fair or poor, while 29% had untreated caries. Suspicious oral lesions were present in 14% (n=308 for the oral lesions indicator), 19% needed immediate dental care and 41% required referral.
Conclusion: This study revealed that surveillance can be accomplished by the collaboration among entities with focus on a specific population. Additional surveillance efforts are warranted among older adults in Illinois in an effort to plan and to implement appropriate interventions for addressing the oral health needs of this population.
Introduction
According to the U.S. Census Bureau, the older adult population is increasing dramatically, with researchers expecting the population of U.S. residents ≥65 years old to increase from 40 million in 2010 to 89 million by 2050, with the population ≥85 years old expected to triple from 5.8 million to 19 million during the same time period.1 Projections indicate 1 in 5 U.S. residents will be 65 or older by 2050, compared with 13% today.1 Demographic data in Illinois mirrors national data, with 13% of the 12.9 million Illinois residents aged 65 and older in 2010.2,3 Surveillance is an integral part of the planning and implementation process for public health intervention;4 therefore, data is needed as an assessment for this rapidly increasing population in all areas of health, not the least of which is oral health.
Identifying the needs of the older adult population, and obtaining a viable database depicting these needs, can help evaluate the current level of and need for oral health services in this population and guide public health policy. The oral health report issued in 2000 by the Surgeon General contained a call for continued research among older Americans and the various oral health issues affecting them.5 At the National Coalition Consensus Conference on Oral Health of Vulnerable Older Adults and Persons with Disabilities,6 the American Dental Association recommended to promote continued research on oral health issues of older adults, as well as the widespread use of surveillance tools like the Association of State Territorial Dental Directors (ASTDD) Basic Screening Survey (BSS) for Older Adults.7
Developing policies and procedures to ensure states engage in appropriate programming for older adults depends upon assessment data to serve as a baseline. Since 2002, Illinois has been developing their Oral Health Surveillance System (IOHSS),8 modeled after the National Oral Health Surveillance System.9 Data was gathered on workforce, decay, sealants, oral cancer and other indicators for the state. However, no oral health surveillance data were gathered for the older adult population. In 2007, Illinois updated an earlier version of its oral health plan to be used as a “roadmap” for future programming in the state.10 Several of the policy goals, recommendations and strategies specifying the older adult population as an underserved group needing specific oral health interventions were referenced in both the Illinois 2007 Oral Health Plan8 and the updated 2012 recently published. Baseline oral health data collection is a necessity for older adults throughout Illinois in order to plan and develop these interventions.
In response to the need to determine a baseline for the senior population, the Illinois Department of Public Health (IDPH), Division of Oral Health (DOH), partnered with IFLOSS (Statewide Oral Health Coalition) and the Illinois dental and dental hygiene schools to compile oral health data on its older adult population. This collaboration developed Smiles Over Time (SOT) 2009-2010, an oral health basic screening survey targeting the 60 years and older population in Illinois. Due to the absence of statewide dental programs addressing this population, this survey was the first step in identifying the oral health status and needs of older adults in Illinois. These data will provide a snap-shot of the challenges and opportunities existing in this population and the ability to track oral health trends for those 60 years of age and older. The assessment report can be used to educate decision makers about oral health needs for senior constituencies, develop policies, plan interventions, leverage resources and implement effective actions.
Methods and Materials
A letter from the IDPH, DOH was sent to the deans, program directors and the community health faculty of the 2 dental and 13 dental hygiene schools in Illinois, inviting them to participate in the surveillance project as a service learning experience in dental public health. The DOH regional oral health consultants followed up with phone calls to schools to answer questions and to verify participation. Many of the dental and dental hygiene schools have established ongoing outreach programs and visit local centers to provide screenings for older adults. The DOH embraced this opportunity to standardize the outreach efforts by the educational institutions. All participation of the schools was voluntary. Institutional Review Board approval to conduct the screenings and compile the data was secured at the state and the educational institution levels.
The SOT survey instrument was based on the methods outlined in the ASTDD 1999 publication Basic Screening Surveys: An Approach to Monitoring Community Oral Health.7 A team consisting of an epidemiologist, IDPH staff and 1 dental faculty developed the screening form for data collection. This form included a questionnaire and an in-mouth screening. The screening form and protocol were sent to all participating schools. Training for all faculty members was accomplished through telephone conferences, and then faculty trained their respective dental and dental hygiene students in basic screening survey protocol.
Each school was allowed to target and select their own older adult service site(s) for survey implementation, as well as including it in their existing curriculum at on-campus clinics to make it easier to add this surveillance-related learning experience to current procedures. The DOH assisted in planning, and the schools contacted the sites to seek permission to perform the surveys. Once the site agreed to participate, the schools integrated the survey into their event planning to assure appropriate notification and permission could be completed by the facilities prior to the screening date. Consent was obtained from all participants prior to screening. Over the course of 5 months, 16 facilities were used as the screening sites for the students and faculties of the respective educational institutions.
Dental and dental hygiene students provided the screenings for the older adults and then the various schools shared the collected data with the DOH. Data was collected on oral hygiene, caries experience, untreated decay, edentulism, soft tissue lesions and the need for urgent care/referral. This project is focused on the data collected on older adults throughout the state excluding participants from the city of Chicago.
The screeners asked the older adults a series of questions and then performed an oral screening. Basic screening survey protocol stipulates a light source and mouth mirror as the only instruments to be used for conducting screenings.7 Criteria for documenting oral hygiene are outlined in Table I.
Untreated Decay
Untreated decay is detected when a screener can readily observe 2 things:
A loss of at least 0.5 mm of tooth structure at the enamel surface (for reference, the ball at the tip of a World Health Organization (WHO) periodontal probe is 0.5 mm in diameter)
Brown to dark-brown coloration of the walls of the lesion
Teeth that meet both of these criteria are considered untreated decay, even if a restoration is also present. If a root is retained, it is assumed that the whole tooth was destroyed by caries.
Treatment Urgency
After assessing each participant according to decay status, 1 of 3 treatment urgency codes was assigned for follow-up care. This was an estimate of how quickly the participant should visit the dentist for clinical diagnosis and any necessary treatment (Table II).
Those participants with no obvious dental problems observed were given a code “0,” which means that they should receive routine dental examinations as recommended by their dentist. The screener could override a code “0” and assign a code “1” if it was believed the participant needed to see a dentist sooner than their next periodic examination.
The screening form was formatted for scanning to facilitate faster input and increase accuracy of recorded information. The name appeared on the survey form to ease tracking documents through the survey process. SOT data was collected by the schools on the standard survey forms provided by the DOH in the spring/summer of 2010. Identifiers were removed from the data. Completed forms were mailed to the DOH. The DOH's data manager scanned the forms into the Teleform software. The MS Access data file was imported to Statistical Package for the Social Sciences (SPSS) for editing and analysis by the epidemiologist. Upon completion, the forms were placed in locked files, stored for 2 years, and then ultimately shredded.
Results
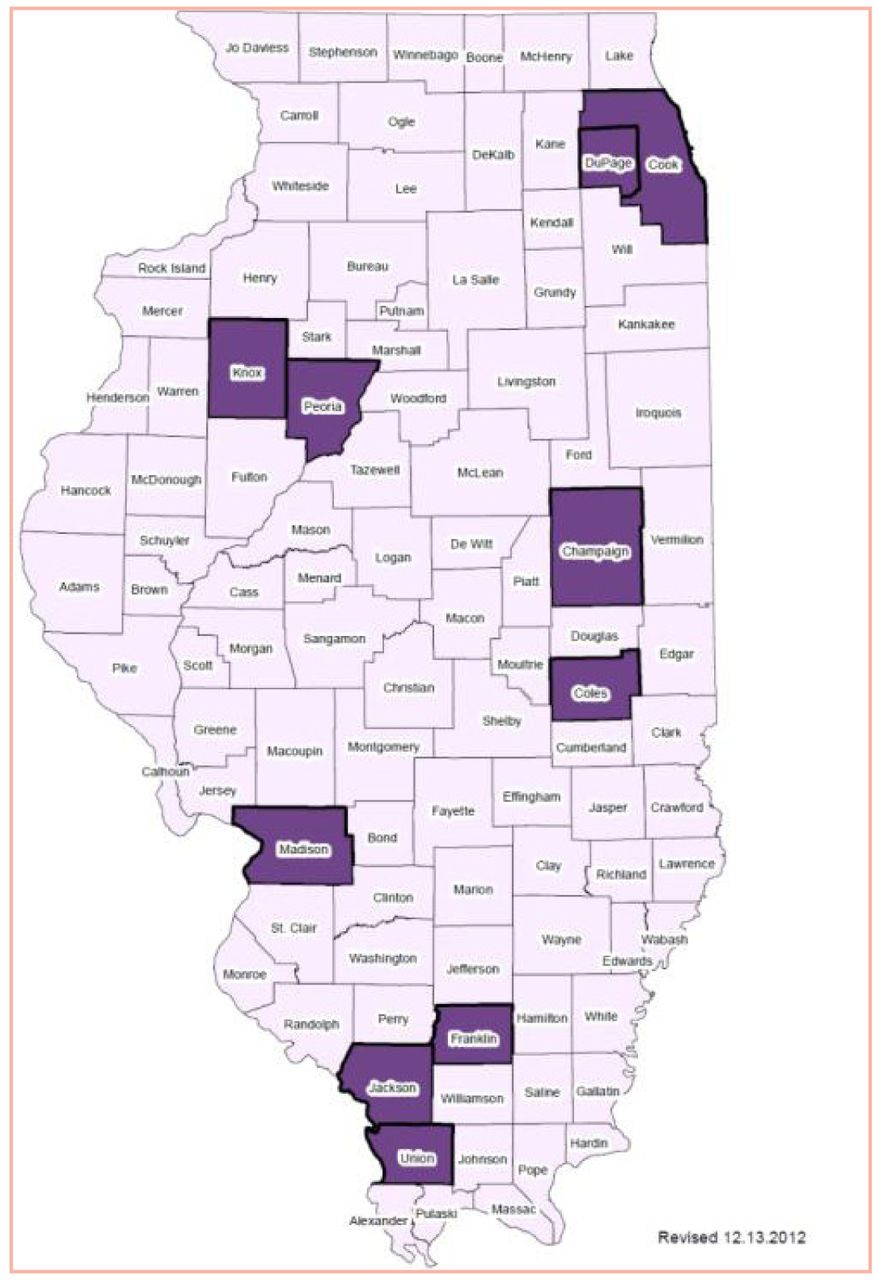
One dental school and 11 dental hygiene schools participated to conduct the oral screenings. A total of 437 older adults were screened at 16 different sites. The sites varied, but 68.6% were screened in a dental hygiene clinic at the various schools. The remainder of the screening sites were a combination of retirement/congregate meal sites, assisted living centers, adult day centers and long term care facilities. The counties in which clients were screened are shown in Figure 1. The average age of participants screened was 75 years, and 67% of the sample was female. Most of the older adults were white. The racial breakdown was 85% white, 6% African-American, 2% Asian and 5% unknown. Screening sites, age distribution, gender and racial breakdown are included in Table III.
All participants were asked a set of questions before the intraoral screening took place. The questions served to document the hygiene habits, frequency of dental care sought by older adults and their access to dental care. Due to the level of dementia affecting older adults, the survey contained a question about the cognizance level of the client as percieved by the survey administrators. A total of 90% were believed to be sufficiently cognizant to provide accurate answers (n=393). The remaining 10% were included in data collection for survey items screeners could assess in spite of limited participant cognitive ability. A total of 53% (211 seniors, n=401), reported having a dentist they visit every year, while 80.8%, (333 seniors, n=412) reported having no dental insurance (Table III). The types of dental insurance carriers reported by the seniors were highly variable and included Medicaid and Medicare.
Criteria For Assessing Oral Hygiene Status
Category and Code to Determine Treatment Urgency
Older adults were asked when they last saw a dentist either at a private office or at the facility where the screening took place. Of those, 58% (243, n=422) reported a dental visit within the last year. The most common reason for the visit was for a check-up, exam or scaling. Approximately 33% (140, n=423) of the clients screened claimed to have some type of denture, and 85% (n=90) claimed they actually wear the denture. Only 40% stated they had received an oral cancer screening in the last 12 months.
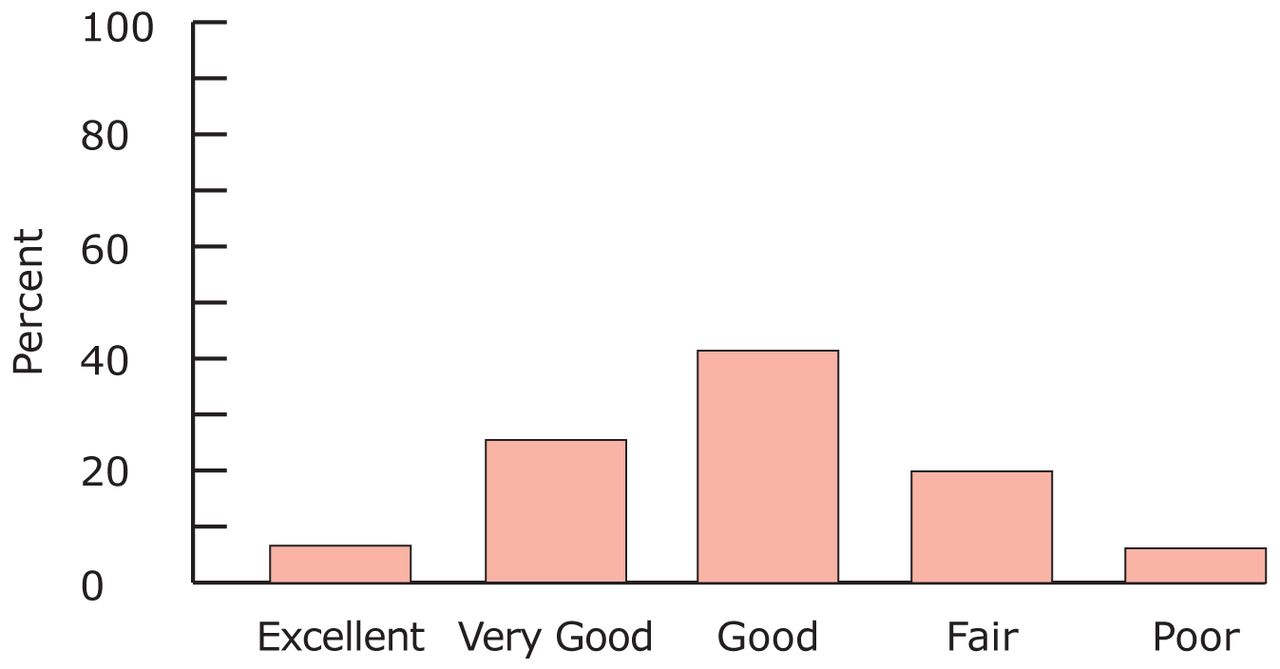
Figure 2 shows the older adults' perception of their oral health status (n=400), with 74% (n=295) rating it as good or better, and 26% (n=105) rating it fair or poor. The most commonly reported site of oral pain (15%) was the gums, with teeth the second most common. A total of 47 of 405 seniors (11.6%) reported bleeding gums in the last week, and 20% reported problems eating or chewing. The majority of clients, 68.6% (n=275), did not notice changes in salivary flow, while 24% (n=96) found it to be too little and 7.5% (n=30) felt an increase. Most of the seniors claimed they were able to brush their own teeth; however, brushing frequency revealed 6% (n=24) brushed less than daily, 37% (n=148) brushed 1 time per day, 47% (n=192) 2 times per day and 9% (34) 3 or more times per day (n=398).
Intraoral health indicators assessed by the screeners were oral hygiene status, untreated decay, soft tissue lesions, edentulism, and the percentage of seniors in need of early and immediate dental treatment. Results are illustrated in Table IV. Screeners rated oral hygiene status (n=414) as excellent for 13.3% (n=55) of participants, good for 38.9% (n=161), fair for 27.5% (n=114) and poor for 18.4% (n=76).
A total of 29% (n=114) had untreated decay (n=394). Suspicious oral lesions were noted for 14.3% (n=44) of the seniors (n=308), and 13% (n=56) of the participants were edentulous (n=430). Nearly 12% had full dentures, 18.8% had a full maxillary denture and 12.4% had a full mandibular denture. Maxillary and mandibular partial dentures were documented for 10.3% and 11%, respectively. For treatment urgency (n=398), 20.6% (n=82) needed early dental care, and 19.3% (n=77) needed immediate dental care. Nearly 41% (n=154) required referral (n=379).
Discussion
The survey instrument developed in Illinois was similar to what has since been developed by ASTDD for states to use for oral health surveillance in older adult populations.7 Results of the assessment provide a good first step in working toward regular basic screening survey efforts among seniors in Illinois.

Counties Where Screenings Took Place
These findings revealed more women than men participated in the screenings. Because it was not a random sample, no conclusions can be drawn by this result; however, this number is consistent with nationwide demographics of older adults in that there are more older adult women than men in the U.S.11 In Illinois, the 2010 older adult census data revealed 12.5% of the population was over 65, with 7.3% women and 5.3% men.12
Based on the 2004 to 2006 IOHSS results, 71% of Illinois adults over age 65 do not have dental insurance.8 The SOT data revealed 81% of those surveyed had no dental insurance. Of those insured, Medicare was listed as one of the carriers, although Medicare does not offer routine dental benefits. It appears the older adults may not fully understand the range of services covered by Medicare or are confused regarding their insurance coverage in general. This could mean the actual number having dental insurance is even lower than demonstrated by the data. The literature is replete with references regarding the lack of dental insurance coverage for older adults.5,13-17 In a 2003 report by Oral Health America, Illinois was given an overall grade of D concerning dental coverage for seniors.13 This grade was issued when Illinois had limited adult dental Medicaid coverage. In 2012, adult Medicaid benefits were reduced even further to primarily emergency and extraction services.18 Lack of insurance coverage is a significant access barrier for older adults across the country and in Illinois.
Older Adult Characteristics by Age, Race, Gender, Type of Screening Facility and Dental Insurance
Utilization of dental services by older adults has increased over the past 50 years and the trend is expected to continue.16,19 Various surveys in 1999, 2002 and 2008 indicate that 50 to 54% of older adults nationally reported having had a dental visit in the previous year.14,16,17 This SOT Illinois assessment showed 58% of older adults claimed to have had a dental visit within the last year compared to IOHSS results of approximately 64%. However, all older adults need an annual dental visit. Several of the Healthy People 2020 oral health objectives speak to decreasing oral disease in older adults.20 Utilization of dental services must increase to move toward achieving the 2020 objectives. This is especially true in respect to oral cancer. Its increased prevalence in older adults makes it imperative for all seniors to access dental services regularly. The dental community must discover how to improve access and enable older adults to utilize dental services to the greatest extent possible.
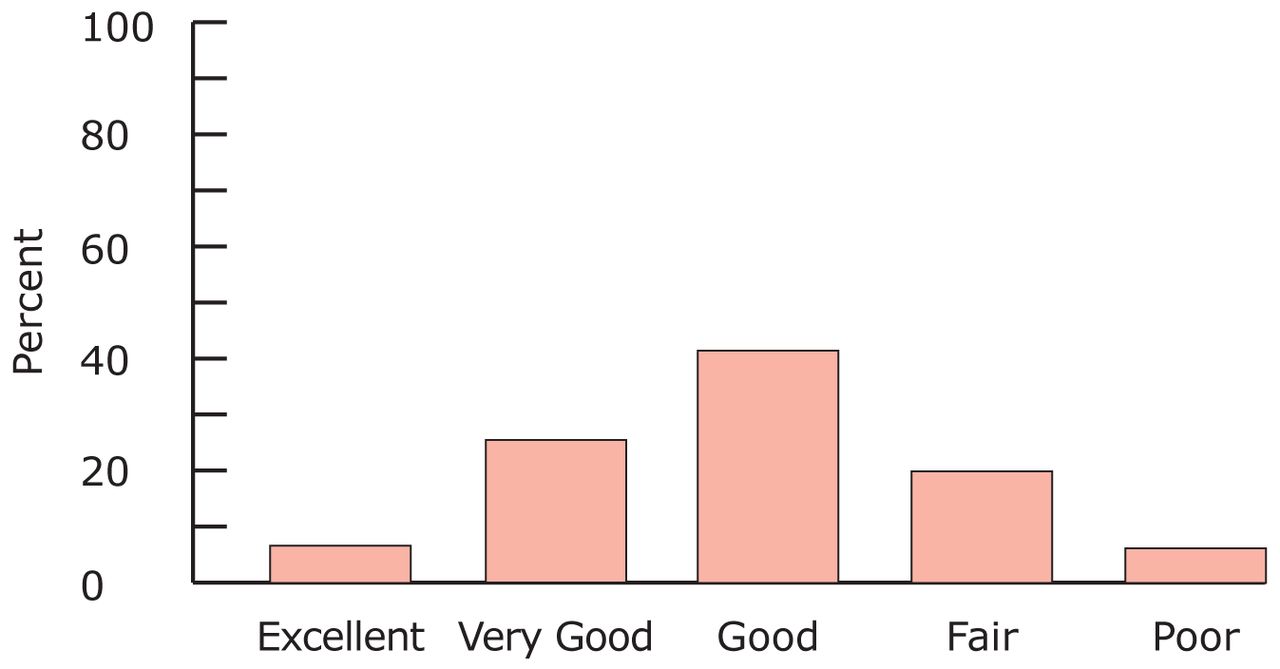
Self Perceived Oral Health Status (n=400)
The number of older adults who are edentulous has declined over the past several years. Based on Illinois Behavioral Risk Factor Surveillance Survey 2003 data, 19% of those 65 years and older had lost all of their teeth, compared to 13% in SOT. Nationally, 18% of 65 years and older were edentulous in 2008.9 The lower rate of edentulism in the Illinois assessment could be due to the fact that 85% of the sample were Caucasian/white older adults. The older adult population is becoming more ethnically diverse. Tooth loss and most other dental diseases are more prevalent in minority populations.5,19,21 Results of the National Health and Nutrition Examination Survey (NHANES) 1999 to 2004 showed African-Americans had a higher prevalence of missing teeth and edentulism than whites and Mexican-Americans. Mexican-Americans had the lowest rate of edentulism of the 3 groups which was contrary to what would be expected for a minority group. The prevalence of edentulism is influenced by multiple factors, including socioeconomic status and the presence of other chronic illnesses.14,21,22 Edentulism varies greatly by state as well. In the 1993 Health Interview Survey, 14 and 16% of older adults in Hawaii and Oregon, respectively, were edentulous, as opposed to West Virginia and Kentucky, which had rates of 44 and 48%, respectively.22 Further research is warranted to determine reasons for edentulism in Illinois older adults.
Intraoral Screening Results
When asked to rate their oral health status, 26% rated it as fair or poor. Studies have indicated older adults tend to perceive their oral health to be better than what it actually is, therefore this may be an underestimation of fair/poor oral health status.23 Several studies also have examined self-perceived oral health status in relation to how it affects quality of life.23-26 Gift and Atchison's research concluded: “oral health is an integral part of general health and contributes to overall health-related quality of life,”24 Locker, Clarke and Payne had similar conclusions.25 A significant proportion of Illinois' older adults may indeed have a lower quality of life due to oral health issues.
It is concerning that 29% (114) of the older adults in this Illinois assessment, most of whom were still mobile, had untreated dental caries. Although caries rates are declining nationally in children, coronal and root caries rates in older adults are increasing.22,27,28 Caries prevalence is even greater in older adult minority populations.5,13,17,22,28 Nationally, minority older adults tend to have more untreated decay than their white counterparts. The SOT untreated decay data was lower than national trends possibly due to the greater proportion of whites than minorities in the sample. As with edentulism, the reasons for increased caries in older adults are many and varied. Efforts to address increased caries in Illinois older adults need further exploration.
The in-mouth survey included an indicator for detecting suspicious oral lesions. Older adults are at increased risk for a variety of oral lesions associated with systemic disease as well as those of oral cancer.29 The American Cancer Society Guidelines for the early detection of oral cancer recommend yearly examinations of the head and neck and oral cavity by health care providers in all asymptomatic men and women age 40 and older.30 In addition, at least once yearly head and neck and oral examinations by dental professionals are required to identify early symptoms of cancers, infections, salivary glandular dysfunctions, oral mucous lesions, bony pathoses and temporomandibular disorders. Older adults with physical and cognitive impairments are more susceptible to developing oral facial pathoses, therefore they must have access to more frequent professional care.31 An interesting finding in this Illinois assessment was of the 437 participants screened, only 308 surveys had the indicator marked for suspicious soft tissue oral lesions. Of those marked, 14.3% or 44 older adults had suspicious lesions as noted by the screeners. The indicator called for a simple yes/no answer on the screening form, not specifying the types of lesions included. Perhaps the persons conducting the screening did not feel comfortable answering for this particular indicator or doubted their skill level of identifying the extent of suspicious lesions. The indicator is not specific for lesions suspected of oral cancer; however, research suggests oral health clinicians do not believe they are well prepared to detect or manage early stage oral cancers and precancers.32,33 This assessment needs follow up with additional screening for Illinois older adults, and screeners should be well trained in lesion identification, especially those suspect for oral cancer.
Other findings of the assessment necessitate comment. For example, 65% had no problems with eating or chewing, but the remaining 35% reported sometimes having difficulty. A portion of the difficulty could be partially from xerostomia, which was reported by 24% and is well documented as an oral health issue in this population.34 Ervin and Dye examined results of NHANES 1999 to 2002 and found a functional dentition (21 or more teeth) did not contribute substantially to nutrient intakes.35 It is not known how the SOT older adults interpreted the question nor what the reasons may have been for their answers. Another finding of SOT was 15% also reported oral pain. This finding could affect results of the question relating to the difficulty with eating/chewing. It could also relate to oral health related quality of life, a relationship that has been the focus of previous research as well.24 Difficulty eating/chewing can be interpreted a number of different ways and requires employing more rigorous methods to determine causes and implications.
The treatment urgency results further emphasizes the need for additional research among older adults in Illinois. It is concerning that 19% needed immediate dental care and 41% required referral. This illustrates that possibly the oral health needs and issues of older adults in Illinois are not being addressed sufficiently and should be examined more closely to encourage policy changes and health promotion, disease prevention and reduction interventions.
Results of the SOT project require cautious interpretation when considering the many limitations of the project. Data was collected by dental and dental hygiene students and checked for accuracy by faculty at most sites. This was not a standard practice for all screenings. When scanned in by IDPH staff, data was missing for several items on the forms. This was partly due to the cognizance level of the older adults, and partly by incomplete data acquisition on the part of the screeners. Self-reported data is often open to scrutiny and especially so in a population identified as having varying degrees of dementia. Nearly all (90%) of the screeners considered the older adults cognizant to answer questions; however, cognitive level of the participants could have been compromised by dementia or memory loss more than what was evident to the screeners during the short time spent with them. This further limits the results of the questionnaire portion of the survey.
Funding was not available for the data collection process, so it was determined that no restrictions could be imposed on those participating to ensure uniformity. All screeners donated their time and services to the project without compensation. The convenience sample results cannot be broadly generalized to include all older adults in Illinois. A small portion of the sample was older adults in long term care facilities, further limiting the generalizability of the results.
Conclusion
The older adult population is increasing with significant oral health issues. Additional surveillance efforts are warranted among older adults in Illinois to be able to plan and implement appropriate interventions for serving their oral health needs. Though not without limitations, this project exemplifies how states without funding earmarked for surveillance activities can still accomplish data collection through collaborative efforts of multiple entities that are concerned with older adult oral health issues. The DOH has routinely designed projects that can be used by schools to enhance dental public health service learning experiences. The SOT project was intended to follow this model. This serves as a good first step in documenting the oral health challenges of and opportunities for planning and implementing programs with the goal of ensuring optimal oral health among all older adults in Illinois.
Footnotes
-
Sherri Lukes, RDH, MS, FAADH, is an Associate Professor Emeritus, Southern Illinois University Dental Hygiene Program, and is also President-elect and Public Health Committee Chair of the Illinois Dental Hygienists' Association. Julie A. Janssen, RDH, MA, is a recent retiree of the Illinois Department of Public Health after 27 years of service. She currently volunteers for IFLOSS, the state wide oral health coalition and is chair of the Central counties health center board of directors. Kathleen K. Thacker, RDH, MPH, is an oral health consultant for the Illinois Department of Public Health, Office of Health Promotion, for the Peoria/Rockford Regions. Sangeeta Wadhawan, DDS, MPH, is a dentist/epidemiologist in Northern Illinois, formerly with the Illinois Department of Public Health.
-
This study supports the NDHRA priority area, Health Promotion/Disease Prevention: Validate and test assessment instruments/strategies/mechanisms that increase health promotion and disease prevention among diverse populations.
- Copyright © 2014 The American Dental Hygienists’ Association





{kind=link}
{kind=link}