



Abstract
Purpose: Lifelong control of disease processes associated with dental caries should be an essential part of the process of care for practicing dental hygienists. The purpose of this study was to identify the knowledge, attitudes and practice behaviors among dental hygienists regarding caries risk assessment (CRA) and management.
Methods: Utilizing the American Dental Hygienists' Association (ADHA) Survey/Research Center database of all registered dental hygienists in the U.S., 2,500 actively licensed dental hygienists were randomly selected and sent a web-based survey via SurveyMonkey™. The survey included items about practice characteristics and questions regarding knowledge, attitudes and practice behaviors regarding CRA and management. Second and third emails were sent to non-respondents. A 4-point Likert type scale (1=never, 2=sometimes, 3=frequently and 4=always) was used to rate the occurrence of caries management recommendations used in the practice setting. Frequencies and percentiles were used to evaluate demographic, knowledge and attitude information.
Results: The response rate was 9% (n=219) - 87% were ADHA members. Participants reported a high level of comfort (89%) in performing CRA, yet only 23% used an established CRA/management instrument. Over-the-counter fluoride dentifrices (70.1%), individualized oral hygiene instructions (86%) and individualized recare intervals (73.7%) were most often used as caries management recommendations, while low-dose fluoride rinses (45%) and prescription strength sodium fluoride gel or paste (42%) were used less frequently. Dental hygienists scored high on knowledge of CRA with the exception of white spot lesions as a risk factor (42%) and efficacy of chlorhexidine in caries management (61%).
Conclusion: There is a need to improve practicing dental hygienists' knowledge and involvement in the active management of caries. Focused training in the use of established CRA/management tools should be designed to improve their knowledge and influence practice behaviors.
- caries risk assessment
- caries management
- white spot lesion
- caries incidence
- dental hygienists' knowledge attitudes and practices
Introduction
Tooth decay is a common, preventable problem for people of all ages. Increasingly over the past decade, dental hygienists have been urged to perform caries risk assessments (CRA) in their practices to increase the probability that patients will receive appropriate caries preventive treatment. In 2003, then Surgeon General Richard H. Carmona sent out a call to action for all oral health professionals to become part of the solution in reducing oral disease and improving oral and general health for all Americans.1 Since that time, statistics on caries disease incidence have shown little change. Caries disease prevalence in children ages 2 to 5 has increased from 24 to 28%.2 Among all adolescents ages 12 to 19, 20% currently have untreated decay. Adults are retaining more teeth and, with the exception of adults ages 50 to 64 who live below the federal poverty level, caries incidence in adults over age 20 has decreased only slightly.3,4 In the modern history of caries management (post-1850), the disease has been treated by surgically removing the infected portion of tooth and replacing it with a restoration, yet this surgical management technique has not modified the bacterial infection or disease process.5 Therefore, more conservative and preventive strategies for managing caries disease have been established.6 Current methods for CRA include a range of objective and subjective methods.
Assessing Caries Risk
Risk assessment procedures used in dentistry should provide sufficient data to accurately quantify a person's disease susceptibility and allow for preventive measures. Risk assessment fosters the treatment of the disease process instead of treating the outcome of the disease, gives an understanding of the disease factors for a specific patient and aids in individualizing preventive discussions, individualizes, selects, and determines frequency of preventive, therapeutic, and restorative treatment for a patient, and anticipates disease progression or stabilization.7 Models of CRA used in the clinical decision making process should include formal components of these assessment characteristics. Clinical management protocols are documents designed to assist in clinical decision-making - they provide criteria regarding diagnosis and treatment and lead to recommended courses of action.
Several tools are available and commonly used for dental caries risk assessment. To understand the differences and similarities in caries risk assessment models, the distinction between risk factors, risk indicators, clinical findings, circumstances and clinical conditions needs to be identified. The terminology varies among the models, but often describes the same factor, clinical sign, etc.8-11 These risk assessment models are adjuncts to the clinical judgment of each clinician, as each clinician has his or her own understanding of caries identification and management protocol.7-11 The Caries-Risk Assessment Tool (CAT) from the American Academy of Pediatric Dentistry (AAPD) is a framework for classifying caries risk in infants, children and adolescents based on a set of clinical findings, protective and biological factors that affect individual dental caries risk.7 The Cariogram® Internet-based program operates in such a way that information on a number of factors – diet, bacteria, susceptibility and circumstances, can be collected on patients of any age.9 Once entered into the program, the information is evaluated and a summary of results illustrating the future chance of avoiding caries becomes available for clinician and patient use. The California Dental Association caries risk assessment forms allow clinicians to assess caries risk of children ages 0 to 5 and for those patients 6 and older.10,11 After identifying risk indicators, risk factors and protective factors, clinicians are able to provide dental caries management protocols specific to the patient 6 years or older or for the parent or primary caregiver of the patient under age 6. The American Dental Association (ADA) caries risk assessment forms were developed to help evaluate caries risk in infants and children ages 0 to 6 and for patients over 6 years of age.8 Clinicians are able to quantify caries risk level at is relates to contributing, general health and clinical conditions. The CRA tools mentioned above are examples of the many methods available to assess and document dental caries risk in clinical settings. All CRA protocols require parent or patient commitment along with anticipatory guidance and a treatment plan.
Caries risk assessment and management protocols should be based on evidence from current peer-reviewed literature, the judgment of expert panels, as well as clinical experience of practitioners.7,12,13 Caries management by risk assessment (CAMBRA) is an evidence-based caries management protocol that gives the clinician management strategies allowing them to make appropriate restorative, therapeutic and preventive recommendations.10,11,13 Once risk level has been established, recommendations of products and protocols will follow, depending on each patient's risk level. Recommendations may take the form of oral self care instructions, antimicrobial use to reduce oral flora, acid neutralizing rinses or sprays, sealants, fluoride varnish, xylitol products and minimally invasive restorative measures.13
Dental Hygienists' Role in CRA/Management
Although clinical responsibilities vary based on individual state's scope of practice rules and regulations, the dental hygienists' role as a prevention specialist is constant throughout regions. Dental hygienists are trained to assess risk, educate and help patients manage and reduce risk for oral diseases.14 Traditionally caries prevention recommendations have included effective brushing, flossing and avoidance of sugary foods, plus twice a year examinations along with fluoride applications. Dental hygienists may take a leadership role in the practice setting by reviewing the literature for development of office protocols in CRA and expanding the preventive and clinical care supplies for caries management. Ultimately, to assess risk, dental hygienists may use a simple, methodical protocol that includes conducting a risk assessment survey, recommending preventive strategies, non-operational, therapeutic procedures, and utilizing additional strategies for patients with special needs. While dental hygienists most likely have undertaken informal, i.e. unrecorded assessments of risk of future caries in individual patients, how they have made these assessments is generally not well understood. There has been no exclusive research in the U.S. on registered dental hygienists' knowledge, attitudes and practice behaviors regarding CRA and management. The entry-level and current practitioner needs to have the knowledge and attitudes necessary to provide the comprehensive care expected in dental hygiene practice today.
The purpose of this study was to identify the current knowledge, attitudes and practice behaviors among registered dental hygienists in the clinical setting involving CRA/management.
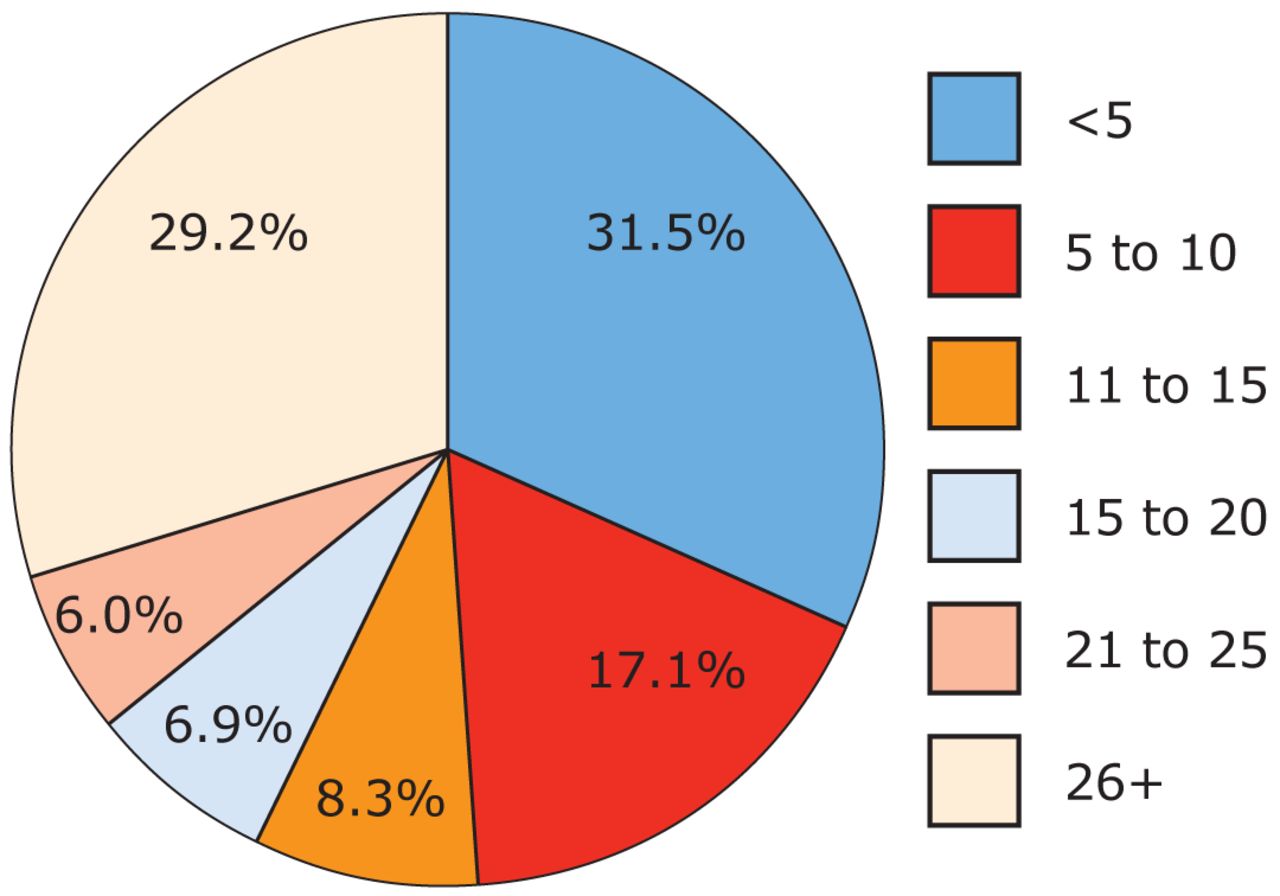
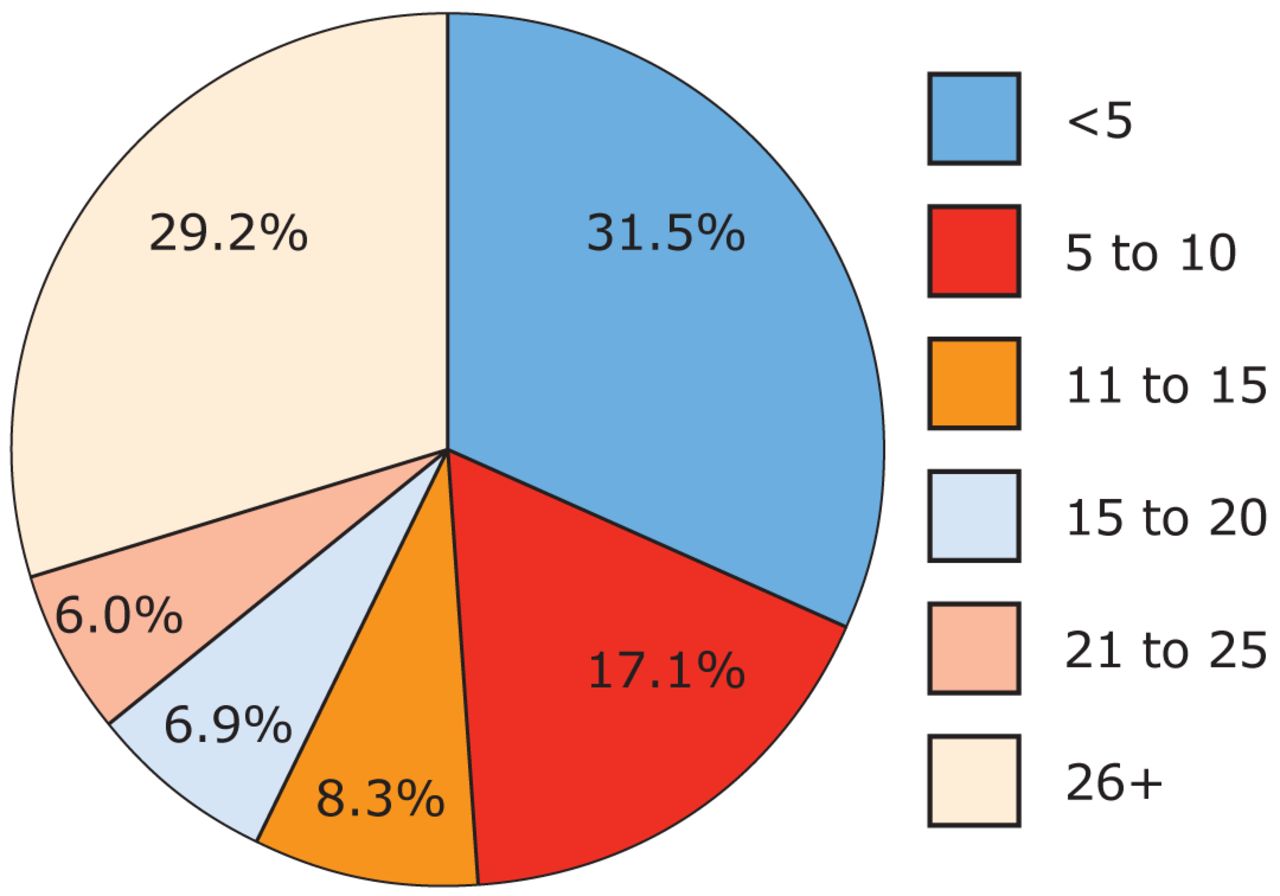
Years since Initial Dental Hygiene Licensure in the U.S. (%)
Methods and Materials
Survey Instrument and Participants
This descriptive study utilized a cross-sectional survey design that quantitatively measured clinical dental hygienists' knowledge, attitudes (comfort and confidence) and practice behaviors regarding CRA and management. The questionnaire included sections designed to assess knowledge (10 true/false items), factors related to performance of CRA in practice (6 agree/disagree items), attitudes encompassing confidence and comfort (5 agree/disagree items) and caries management recommendations (2 items). A 4-point Likert type scale (1=never, 2=sometimes, 3=frequently and 4=always) was used to rate the occurrence of caries management recommendations used in the practice setting. Evidence-based factors that affect caries disease risk were used to develop the questionnaire. The use of chlorhexidine, xylitol and amorphous calcium phosphate products were included, though research on their efficacy in caries management is ongoing and current level of use is unknown.15-17 A sixth section assessed professional characteristics and demographics.
Approval for the survey was secured from the Idaho State University Institutional Review Board. A dentist and dental hygienist, both experts in cariology, evaluated the survey instrument for content validity. Confusing verbiage, clarity and typographic issues were identified and corrected. The survey was then administered to dental hygiene faculty (n=8) at the University of the Pacific Arthur A. Dugoni School of Dentistry to determine instrument reliability using the test-retest method.18 Wording was changed for clarity. An additional 4 clinically practicing dental hygienists pilot tested to assess time needed to complete and readability of questions. No further changes were made at as a result of the pilot test.

Reported Number of Hours of Caries Assessment Coninuing Education Within Past 5 Years
Utilizing the ADHA Survey/Research Center database of all registered dental hygienists in the U.S., 2,500 actively licensed dental hygienists were randomly selected and sent a Web-based survey, via SurveyMonkey™. Instructions to participants reminded them of their anonymity with regard to survey responses. Second and third emails were sent to nonrespondents.
Statistical Analysis
Frequencies and percentiles were used to evaluate the demographic, knowledge, attitude and risk assessment and management techniques. The Spearman rank correlation coefficient was used to identify if knowledge and attitudes (comfort and confidence) were related. Statistical analysis was completed using the SPSS Statistical 19.0.0.
Results
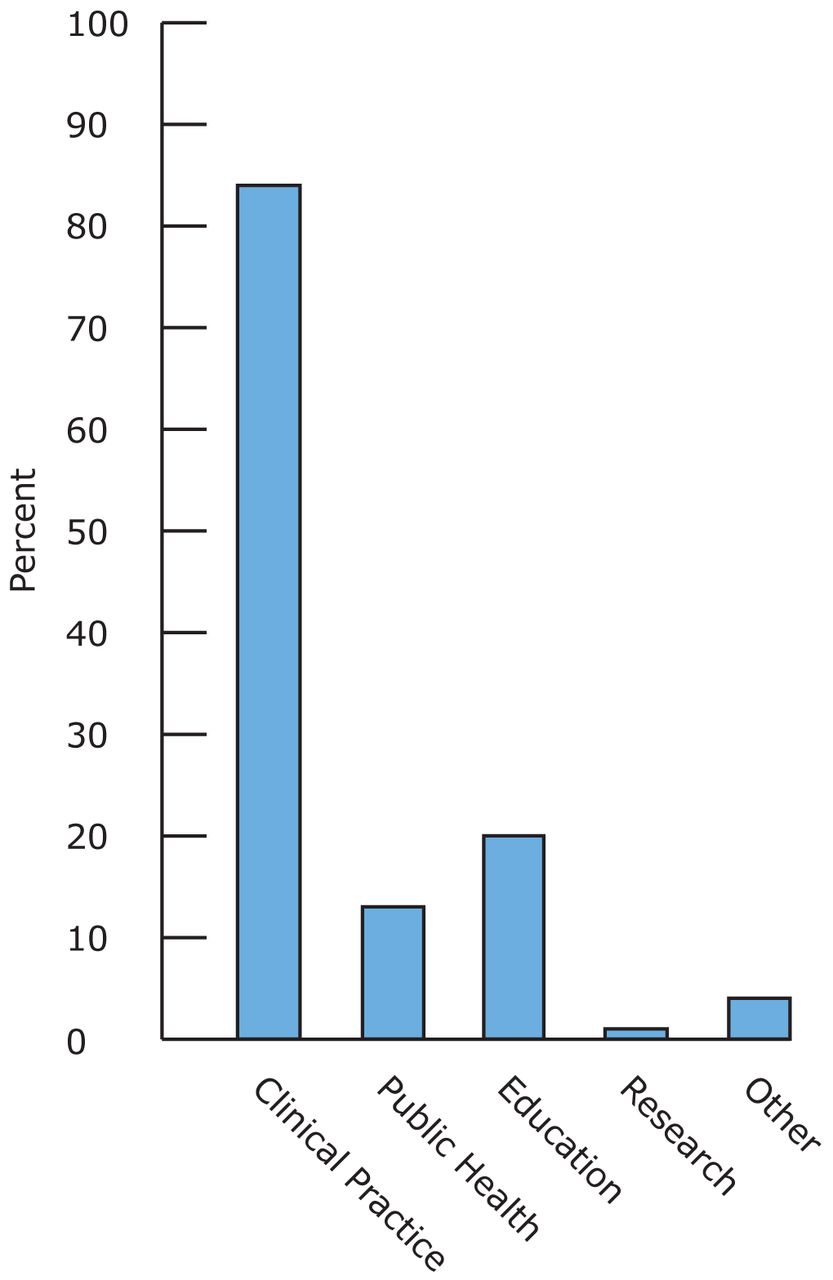
Of the 2,500 email surveys sent, only 216 were valid for analysis resulting in a response rate of 9%. Surveys with missing data were excluded. A total of 88% (n=190) of respondents were ADHA members, 31% were between 25 to 34 years of age and 61% were between 35 and 64 years old. A total of 32% of participants (n=68) reported having received licensure within the past 5 years, 39% (n=83) between 6 to 25 years and 29% (n=63) for over 26 years. Figure 1 shows the years since licensure of the survey participants. Figure 2 shows the hours of continuing education (CE) in CRA in the previous 5 years. A total of 86% of respondents (n=186) see patients of all ages in their primary dental hygiene practice setting. In addition to practicing in a clinical setting, other practice settings cited included educational and public health settings. Figure 3 lists the clinical practice settings noted by respondents.
Knowledge Scores
Knowledge scores were high, with 77% (n=167) having 8 or more correct answers out of 10. Participants correctly identified caries as a transmissible disease (86%) and recognized the multifactorial nature of the disease (98%). History of caries lesions in the last 3 years, low socioeconomic status and reduced saliva flow were correctly identified as increasing risk for caries disease by 88, 86 and 99% of the respondents, respectively. Between 82 and 99% recognized fluoride varnish, xylitol and dietary counseling as factors reducing caries risk. Only 42% (n=90) of dental hygienists identified white spot lesions as incipient caries in enamel, and 60% (n=131) recognized chlorhexidine (CHX) (Peridex; 3M ESPE, Minneapolis, Minn.) as not being bacteriostatic or bacteriocidal to all caries pathogens (Table I).
Attitude (Confidence, Comfort) Scores
The vast majority (89 to 97%) of participants noted being comfortable and confident performing caries risk assessment in their primary clinical practice on all ages of patients, including those with special needs. Cronbach's alpha reliability coefficient was 0.76 for internal consistency of comfort with performing CRA. A total of 71% (n=154) felt they had enough time during an appointment to conduct a CRA and provide management recommendations. Respondents overwhelmingly felt confident in detecting incipient caries in their earliest stages (93%) and comfortable explaining CRA/management protocols (96%) to patients. However, 25% (n=53) affirmed caries management consisted primarily of restorative care (Table II).
Practice Behaviors
Out of 216 respondents, 29% (n=62) used established forms to conduct CRA. Of those, 39% (n=24) used the established form employed the American Academy of Pediatric Dentists' Caries-risk Assessment Tool (AAPD CAT), 22% (n=14) used either the ADA or California Dental Association CRA forms, and another 39% (n=24) used other forms not listed in the survey. The remaining respondents 71% (n=154) stated no formal means of CRA were used. Participants were asked to describe evidence-based caries management products and protocols they use during care when making recommendations to patients at moderate or high risk. Over-the-counter fluoride dentifrice (70%), individualized oral hygiene instruction (86%) and an individualized recare interval (74%) were the most-used caries management recommendations. Low-dose fluoride rinses (45%) and prescription strength sodium fluoride gel or paste (42%) were less frequently suggested as caries management practices and amorphous calcium phosphate products and xylitol gum, mints or lozenges were either never (22 and 9%, respectively) or only sometimes (38 and 35%, respectively) proposed. Table III details the responses regarding use of caries management recommendations.
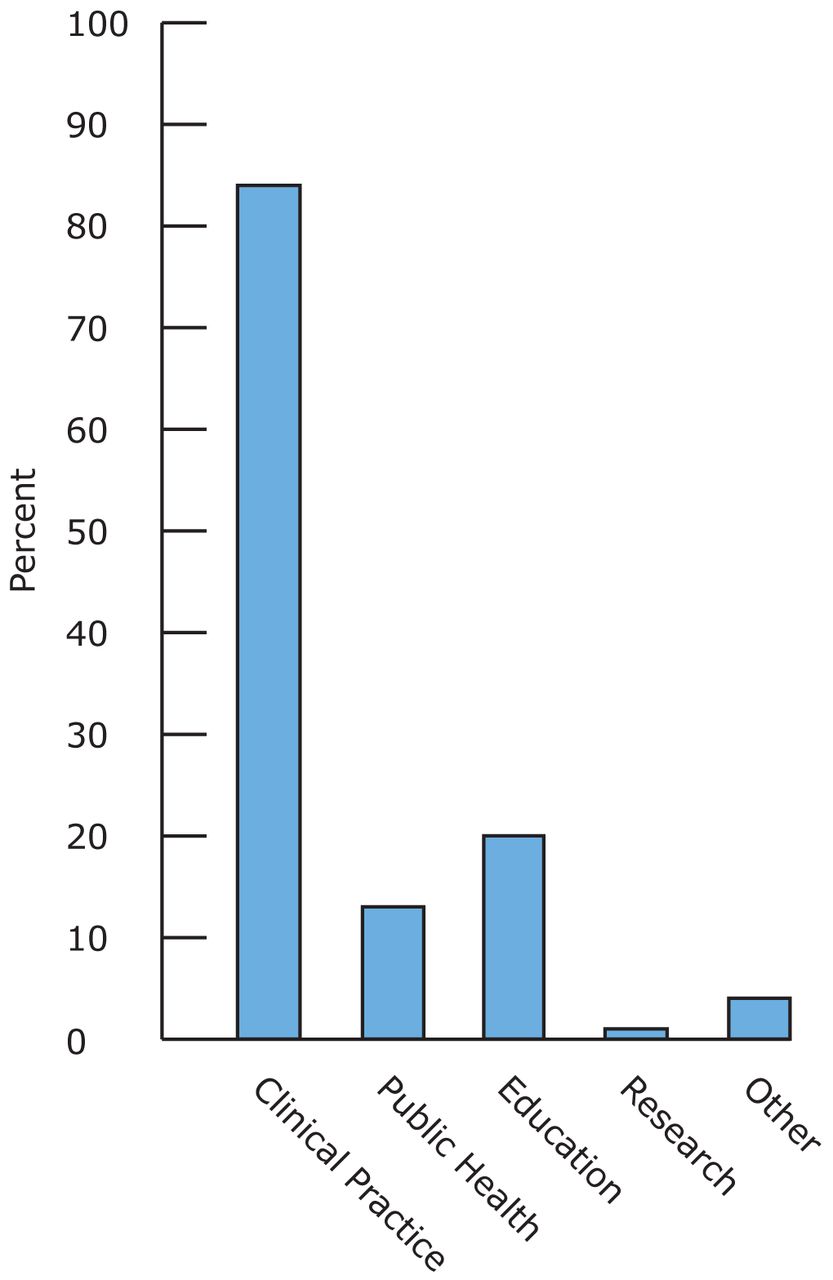
Practice Settings noted in Percentages
Discussion
Dental hygienists, as the primary preventive specialists of the dental team, are in a unique position to implement office based CRA/management programs. Risk assessment and management involving dental hygienists could positively impact or eliminate caries disease across all age ranges. This study provides baseline information necessary to better understand the current level of knowledge, attitudes (comfort and confidence) and practice behaviors concerning CRA and management by dental hygienists. Results indicate that the median age range of respondents was between 25 to 34 years of age, similar to national statistics on age of licensed dental hygienists. Unlike national statistics on dental hygiene practitioners, where the median number of years in practice is 17, over half surveyed had been licensed for less than 5 years (31.8%) or more than 26 years (29.4%), 10 being the median number of years since licensure.19 According to a 2007 ADHA Survey of Dental Hygienists, there were approximately 152,000 licensed dental hygienists in the U.S. and an estimated 130,000 (85.8%) were actively practicing.19 Nevertheless, only 35,000 (23%) of currently licensed dental hygienists are ADHA members, a significant difference from respondents of this survey. Of those who responded, 87% were members of the ADHA, indicating the participants were not a representative sample of dental hygienists nationwide. Figure 4 shows the comparison between professional membership of respondents and dental hygienists nationwide. Respondents' membership in the ADHA may have been beneficial in their knowledge and use of evidence based CRA and management protocols.
Dental Hygienists' Knowledge of CRA/Management
Factors Influencing Utilization of Caries Risk Assessment
In this study, the most frequently used preventive approaches in caries management were recommending over-the-counter fluoride dentifrices, individualizing oral hygiene instruction and setting an individualized recare interval based on dental caries risk. Consistent use of prescription fluoride paste or gel is a key strategy for those at moderate to high risk for caries, yet less than half of respondents reported making this recommendation in their practice setting.20 Given the critical role of fluoride in the prevention and management of caries, these results suggest a need to update dental hygienists in the most effective, evidence-based protocols in the management of caries disease across all age groups. Although the majority of respondents recognized that dental caries management encompasses more than restoring the consequences of caries, 25% reported management to be traditional restorative care. This may result in great variability between the need for risk-based caries management and prevention and how practitioners apply these concepts in private and community settings. Fewer than half of responding hygienists considered evidence of incipient cavitation (white spot lesions) to be a significant risk indicator for caries. White spot lesions are described as the beginning of the caries lesion - the point at which demineralization outpaces remineralization and the enamel surface begins to weaken.16,21,22 Clinical evidence shows that the early stages of demineralization may be reversible following exposure to fluoride, and treating incipient caries lesions with fluoride is the hallmark of non-invasive remineralization therapy.21,22 Thus, dental hygienists need to be more familiar with the earliest stages of caries disease, as reflected by this study.
Dental Hygienists' CRA Management Recommendations
Data indicated participants' attitudes (confidence and comfort) about carrying out CRA for all age groups, including those with special needs, to be quite high. A larger than anticipated number of respondents (71%) felt they had sufficient time to assess caries during an appointment. This finding is surprising, considering the number of dental professionals citing time as a barrier to the incorporation of evidence-based decision making into clinical care as well as locating resources.23,24 However, recent advances in electronic access to information and resources have enabled practitioners to implement many evidence-based protocols into care.
The use of 1 of the 4 established forms listed on the survey — AAPD CAT, ADA, California Dental Association and Cariogram®, or a variation, combination or modification of established forms, was reported by 29% of participants. This finding is not alarming considering the variety of forms and risk assessment systems available to clinicians today. Though the Cariogram® caries risk assessment model has been validated in several small studies, only the California Dental Association caries risk assessment form for ages 6 to adult has been validated through a 6 year large retrospective study.12,25 Currently used CRA forms or variations of established protocols are an important part of assessing and documenting current oral health status of each patient. Clinicians should look carefully at the variety of forms available to determine which best fits the need of each clinical setting. Terminology varies among the CRA forms and systems. Ease of use, need to adapt to computerization, target population and terminology consistent with the office philosophy will help dentists and dental hygienists choose the most useful tool. Current CRA methods should measure risk at the earliest possible stage.
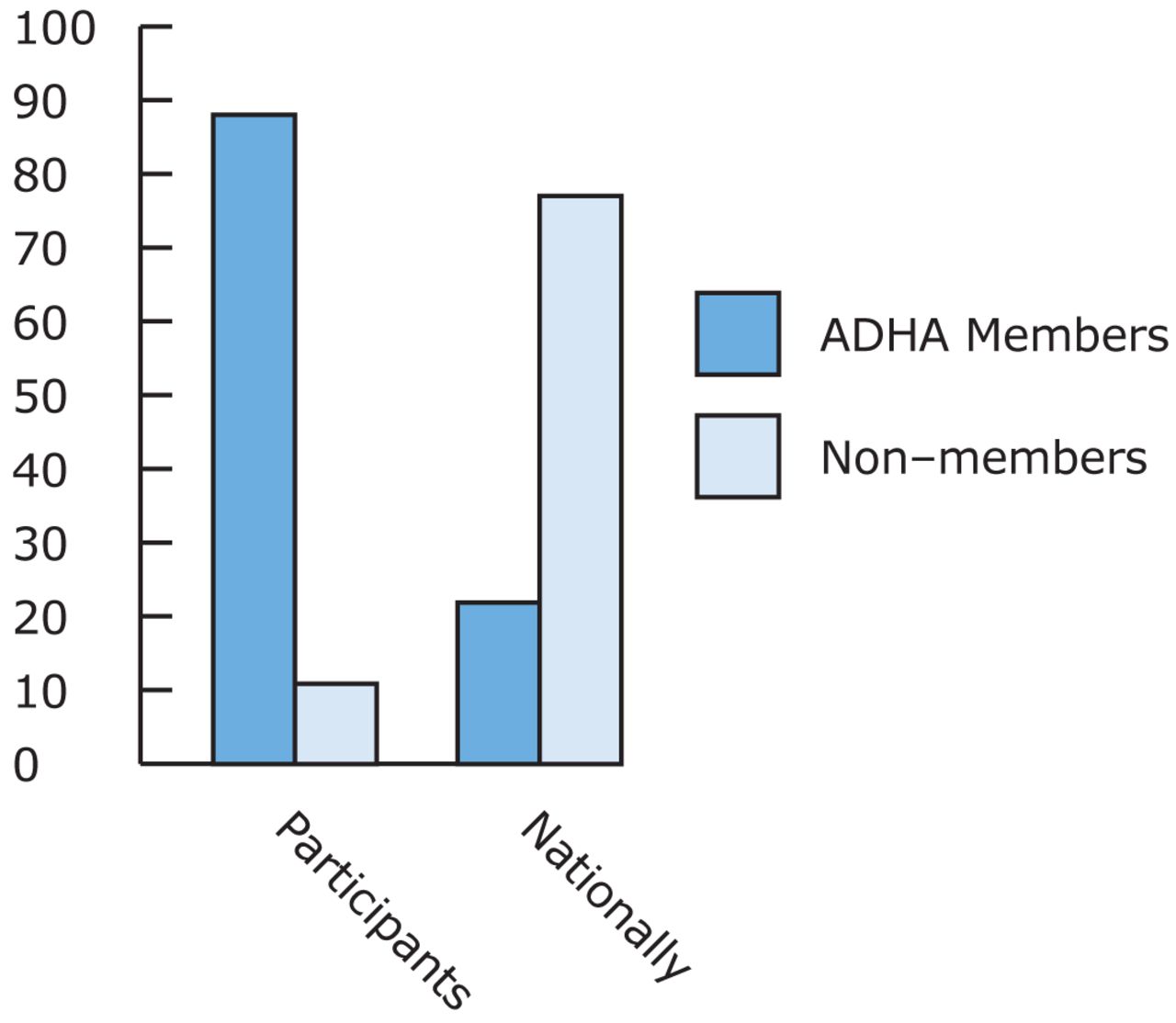
Percentage of ADHA members nationwide compared with survey participants
While providing insight and useful baseline data, limitations to this study must be taken into account. The survey described only reported behaviors and practices, and answers were normative, rather than actual. Although participants selected to participate in this survey were randomly sampled, self-selection bias was a limitation. That is, dental hygienists who chose to respond to the survey may have been different than those who did not respond, thus biasing the results. While the survey provided descriptive data on knowledge and attitudes regarding CRA and management, the instrument lacked the flexibility to uncover the basis for such attitudes. Finally, response rate to the survey was extremely low. Those who responded to the survey were not a representative sample of dental hygienists nationwide. Therefore, results cannot be generalized to the total population. The valid response rate was 8.6% of the 2,500 email addresses targeted. Few national online surveys of practicing dental hygienists have been published for comparison. Of those published, response rates were significantly higher, perhaps due to different sampling methods, or those surveyed may have had increased interest in the topic.26,27 Topic saliency has been shown to contribute to low response rate.28 Research has shown, if interest in the topic is high, response rates tend to be high as well.29,30 Conversely, low response rates may reflect a low perceived interest in the topic. Dental hygiene clinicians who do not routinely perform CRA in practice may have not responded to a survey of this nature.30 Findings from meta-analyses of the literature on survey response rates indicate web-based surveys tend to have lower response rates than mailed surveys, possibly reflecting participants' comfort level with computer technology.30-32
Conclusion
Clearly, there is a need for further research to identify and validate CRA strategies that can be applied in dental hygiene practice. More importantly, studies are required to establish whether identification of moderate and high-risk individuals can lead to more effective long-term patient management that arrests or reverses the progression of carious lesions. Dental professionals must recognize and accept that the process of caries diagnosis today is more complex and involves thorough evaluation of known disease indicators and risk factors, a CRA, microbial measurements, radiographic evidence, and knowledge of the patient's medical and oral health histories. There is a need to improve practicing dental hygienists' knowledge and involvement in the active management of caries. Focused training in the use of established CRA/management tools should be designed to improve their knowledge and enhance practice behaviors.
Acknowledgments
The authors thank Teri Peterson, Statistician Consultant, Michelle Hurlbutt, RDH, MS, and Douglas Young, DDS, PhD, for their expert assistance.
Footnotes
-
Elena M. Francisco, RDH, BSDH, is a Clinical Instructor in the Department of Dental Hygiene at the University of the Pacific, Arthur A. Dugoni School of Dentistry. Tara L. Johnson, RDH, PhD, is an Assistant Professor in the Department of Dental Hygiene, Division of Health Sciences at Idaho State University. Jacqueline J. Freudenthal, RDH, MHE, is an Associate Professor in the Department of Dental Hygiene, Division of Health Sciences at Idaho State University. Galen Louis, PhD, is the Director of the Public Health Program, Idaho State University.
-
This study supports the NDHRA priority area, Clinical Dental Hygiene Care: Investigate how dental hygienists use emerging science to reduce risk in susceptible patients (risk reduction strategies).
- Copyright © 2013 The American Dental Hygienists’ Association





{kind=link}
{kind=link}
{kind=link}
{kind=link}