



Abstract
Purpose Disaster victim identification (DVI) service requires knowledge, confidence, and an attitude (KCA) of readiness. The purpose of this study was to assess allied dental students’ perceived KCA regarding DVI skills and topics.
Methods A convenience sample of senior dental hygiene students (n=27) and senior dental assistant students (n=14) were recruited by email then presented mismatched simulated antemortem (AM) and postmortem (PM) bitewing radiographs and asked to indicate correct matches. Collectively, participants made 205 radiographic matches and indicated 205 degrees of certainty binarily as “positive” or “possible” (one per match). Participants also completed a researcher designed pretest/posttest electronic survey with seven 3-point Likert-scale items with answer options of “slightly”, “moderately”, or “extremely” regarding self-perceived knowledge. Statistical analyses were conducted with R software using an α=0.05 significance level.
Results A total of n=41 students participated, yielding a response rate of 85.4%. A one-sided linear trend test revealed statistically significant increases of perceived confidence in knowledge from pretest to posttest regarding forensic odontologists’ role in DVI (p<0.0001), DVI applications for mass fatality incidents (MFI) (p<0.0001), role of dental radiology in DVI (p<0.0001), and dental morphology applications for DVI (p<0.0001). Participants indicated moderate or extreme confidence in personal clinical skillsets to assist forensic odontologists with DVI. A one-sided Fisher’s exact test revealed a statistically significant (p<0.05) positive association between expressed degree of certainty (confidence) and correct radiographic matches. A one-sided linear trend test revealed statistically significant (p<0.0001) improvements in attitude regarding participants’ perceived importance for their respective professions to volunteer in DVI.
Conclusion Participants of this study reported significant improvements of self-perceived KCA regarding DVI skills and topics. These characteristics may encourage allied dental professionals to pursue further DVI educational opportunities and future service when support is needed for MFI.
- dental hygiene students
- dental assistant students
- disaster victim identification
- forensic odontology
- dental radiology
INTRODUCTION
Natural and man-made mass fatality incidents (MFIs) can occur anywhere and anytime, creating an overwhelming demand for disaster victim identification (DVI) of human remains. Large MFIs which supersede the availability of medical examiners/coroners and forensic odontologists, require support by supplemental personnel with specialized skills including allied dental professionals.1 Registered dental hygienists and dental assistants recruited as service volunteers have supported forensic odontologists in human identification efforts for decedents from sources including civilian and military morgues, transportation crashes, accidental fires, terrorist attacks, and disasters related to weather.2-7 It is important to identify the cognitive abilities to perform the required skills as well as the affective domain attitudes needed for such activities by potential DVI volunteers. Doing so will help identify potential barriers and best practices for response implementation.
Dental hygiene and dental assisting graduates of programs accredited by the Commission on Dental Accreditation (CODA) are deemed competent for clinical practice in their respective disciplines as a result of successful completion of didactic, laboratory, and patient care;4,8-10 content and competencies that are closely aligned with forensic odontology curricula.4,11 When paired with forensic odontologists, allied dental professionals are ideal for supporting the efficiency and success of DVI efforts due to their dental related expertise and have been shown to outperform volunteers without dental related education.9-10,12-17 Regardless of one’s dental background, special DVI training is needed prior to serving on DVI teams.1-2,18 This public service opportunity creates a need for evidence-based educational interventions and assessments to develop and measure cognitive and affective outcomes established in the formal curriculum and/or early in the profession.
The American Board of Forensic Odontology’s (ABFO) Model of Curricular Topics for forensic odontology includes: anatomy, histo-embryology, dental radiology, pathology, and dental materials as foundational subjects necessary for human identifications.19 These five curricular topics are closely aligned with the American Dental Education Association’s (ADEA) Compendium of curricular guidelines for dental hygiene and dental assisting formal education.20 Despite the relational interconnectedness and relevance of forensics for allied dental professionals, this topic is rarely part of the curricula and special training is not widespread.18 One study of dental hygiene students found that graduating seniors were successful in match accuracy of antemortem (AM) and postmortem (PM) images with varying amounts of clinically detectable dental identifiers (CDDI),18 a critical skill used by DVI volunteer consultants for the reconciliation phase.21 The DVI reconciliation phase examines and compares multifactorial AM and PM data and is heavily reliant on quality AM dental evidence developed with strict adherence to state laws and dental industry standards and guidelines for record keeping.1,12,22-24 Though dentists are responsible for the oversight of patient care and record keeping, these are often the product of work performed by dental hygienists and dental assistants.18, 23, 25
Dental hygienists typically perform an initial visual examination and interpretation of typical and atypical findings on dental radiographs of live patients. This is a transferrable DVI skill which is useful for consultation purposes with a forensic odontology section chief who may be attempting to establish a degree of certainty for a report of findings, recommendations, and conclusions regarding human identifications.18
The ABFO has created degrees of certainty or identification scales for body identification (Table I).17,26,27 Forensic odontologists use these standardized terms to communicate the level of certainty or confidence for an identification match based on consistency for concordant points when comparing AM and PM data.27 It has been suggested expressed confidence may be affected by cognitive biases, including being over-confident, which threatens the validity of forensic decisions.27 Radiographic interpretation, part of the dental hygienists’ scope of practice, is critical for the DVI team ability to form conclusions on AM and PM radiographic data.18 Allied dental health professionals should be well prepared to volunteer in DVI efforts. The purpose of this two-part study was to assess dental hygiene and dental assistant students’ perceived knowledge, confidence, and attitudes related to DVI following a multimedia learning experience and radiographic match accuracy activity.
ABFO Degrees of Certainty26
METHODS
Approval from Old Dominion University and Metropolitan Penn Valley Community College Institutional Review Boards (IRB Exempt Status: #1693121-4) was obtained prior to beginning this study. A convenience sample (n=48) of senior dental hygiene students attending Old Dominion University and senior dental assisting students from Metropolitan Community College, Penn Valley were invited to participate in an online learning experience on DVI. Informed consent was sent via email and each participant was required to create a unique identifier to maintain anonymity, prior to beginning the study.
Students who consented to participate were provided the pretest survey, learning experience, and posttest survey with explicit directions for each step. The surveys were delivered via an online platform (Qualtrics; Provo, UT, USA). As an incentive, respondents were given the option to enter a raffle to win one of four gift cards from an online retailer.
The investigator designed pretest survey consisted of seven 3-point Likert-scale questions, which asked respondents to indicate their perceived levels of agreement as “slightly”, “moderately”, and “extremely” regarding DVI topics including their understanding of the scope of forensic odontology, who a forensic odontologist is, the application of DVI in MFIs, understanding of how oral radiology and morphology are used in DVI, confidence to assist with forensic odontology, and the importance of assisting in future DVI when needed. Additionally, five demographic information questions asked participants to indicate their program type (dental hygiene or dental assisting), age, gender, race, and whether they had any prior forensic odontology curriculum at their respective institution.
The multimedia learning experience consisted of a 15-slide presentation with educational text, audio/video recordings, and simulated AM and PM radiographs. This learning experience was presented in a virtual asynchronous format by one of the researchers. Immediately following the learning experience, participants completed a posttest survey asking the same seven 3-point Likert-scale questions from the pretest survey, to assess any cognitive and affective changes resulting from exposure to the learning experience. A radiographic match assessment, including forced binary selection of degree of certainty for the matches was also completed as part of the posttest survey. To gain insight regarding how confidence might be affected by the amount of challenge posed by the radiographs, participants were provided four bitewing (BWX) sets defined as “challenging” (consisting of 0-10 visual CDDI), and one set defined as “less challenging” (consisting of more than 10 CDDI). The detailed research design and method for data collection of participants’ match accuracy have been described previously.28 Statistical analysis was performed in “R” software using descriptive statistics, tests for association such as Fisher’s exact test, and linear trend test based. The significance level was set at α=0.05.
RESULTS
A total of 27 dental hygiene students and 14 dental assistant students consented to participate, for a response rate of 85.4% (n=41). All participants were female (100%) and most (51.2%, n=21) were 18-22 years old and self-identified as White (58.5%, n=24). The demographics of the study population are shown in Table II.
Demographics
Confidence in DVI Knowledge
Following completion of the multimedia experience, participants indicated perceived confidence in their knowledge of DVI concepts of four Likert scale questions with response options ordered as slightly (low understanding level), moderately (average understanding level), and extremely (high understanding level) (Table III). A contingency table was created for each item, ordered scores were assigned to categories, and questions were tested individually with a one-sided linear trend test where the degree of linear trend was measured using sample correlation coefficient. Results revealed statistically significant increases of perceived confidence in knowledge from pretest to posttest for the following: who a forensic odontologist was and their role in DVI (degree of linear trend, R=0.596, 95% C.I.=(0.378, 0.814), p-value<0.0001), the application of DVI used in MFIs (R=0.672, 95% C.I.=(0.454, 0.890), p<0.0001), how dental radiology is used in DVI (R=0.586, 95% C.I.=(0.368, 0.804), p<0.0001), and how dental morphology is applied to DVI (R=0.601, 95% C.I.=(0.383, 0.819), p<0.0001). Table III breaks down each question based on the number of responses for each response level. Additionally, participants were asked on the posttest to rate the confidence of their clinical skillsets to assist forensic odontologists with DVI. Collectively, participants responded as slightly confident (7.3%), moderately confident (56.1%), and extremely confident (36.5%).
Levels of perceived knowledge related to DVI topics
Degree of Certainty with Match Accuracy
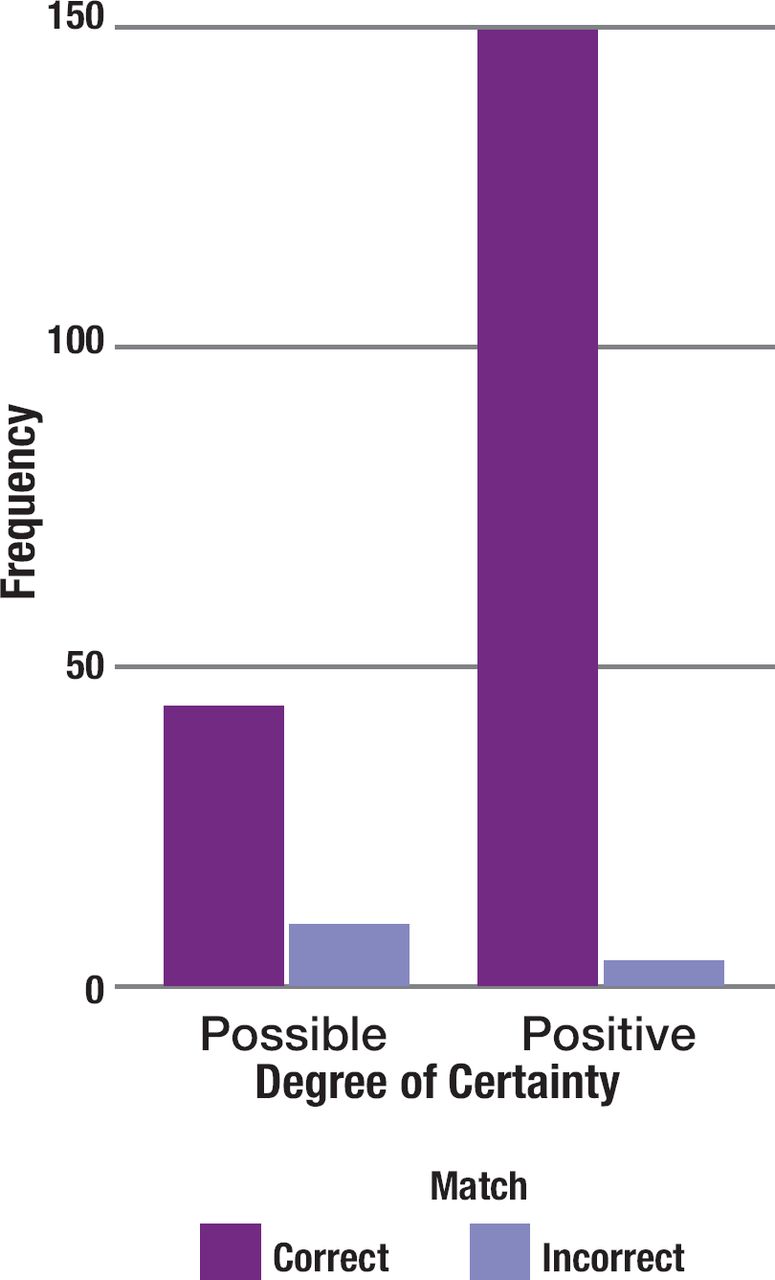
Participants made a total of 205 matches for the radiographs and then indicated 205 degrees of certainty as either “positive” or “possible” (one per match) to determine the association between match accuracy and degree of certainty. A one-sided Fisher’s exact test was utilized for testing the null hypothesis that there would be no association between degree of certainty and radiographic match accuracy against the alternative hypothesis that there would be a positive association. A p-value less than 0.05 revealed a statistically significant positive association between participants’ report of a “positive” degree of certainty and their correct matches of radiographs. Therefore, among these participants, the odds of having a correct match were greater when participants indicated a “positive” degree of certainty compared to a “possible” degree of certainty (Figure 1).

Correlation of student confidence and radiographic match accuracy
Additionally, each participant was tested five times by making five individual identification radiographic matches. The Fleiss’s Kappa intra-rater reliability estimate for the participants is 0.203 (95% C.I.=(0.107, 0.300)). Since 95% confidence interval for the Fleiss’s Kappa statistic suggests a statistically significant level of agreement among the participants, which supports a positive intra-rater reliability for each participant.
Importance of Future DVI Volunteerism
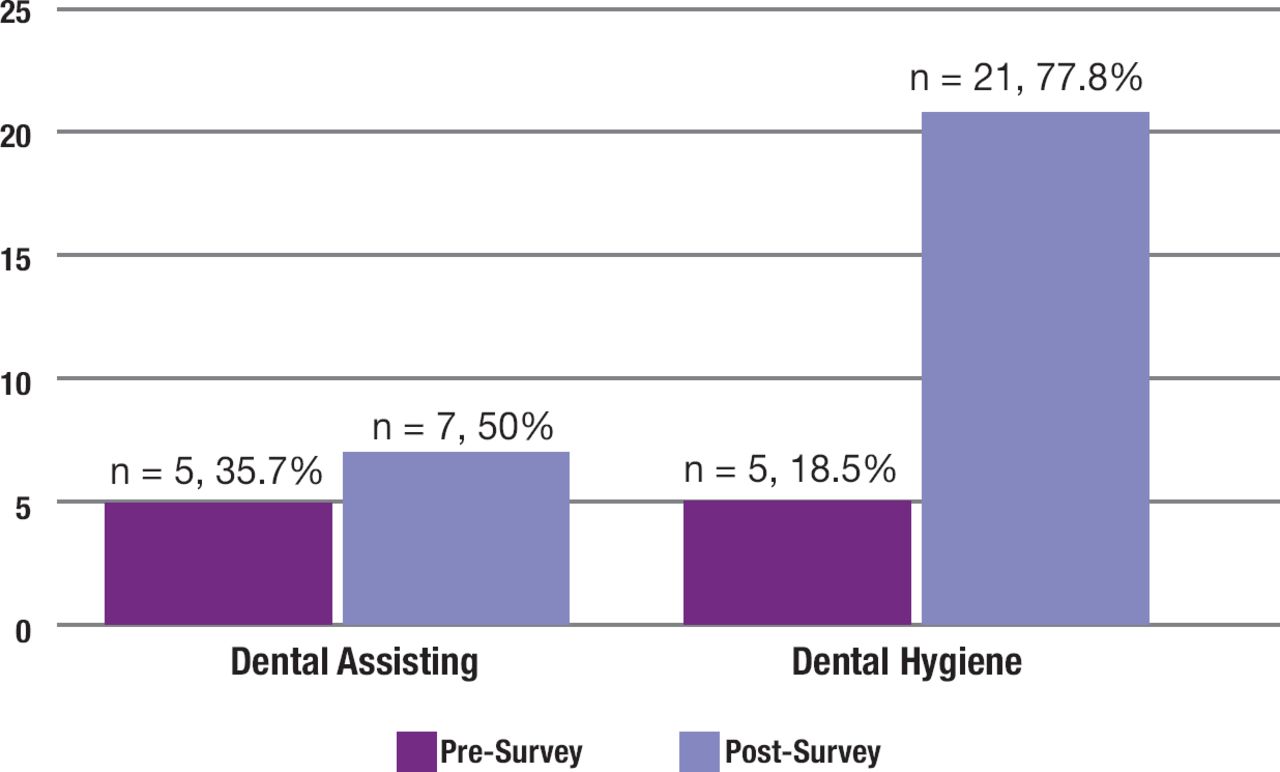
A linear trend test analyzed students’ pretest/posttest attitudes regarding perceived importance for their respective professions, dental assisting or dental hygiene, to volunteer in DVI and revealed a statistically significant improvement in attitude upon completion of the learning experience (R=0.486, 95% C.I.=(0.286, 0.704), p<0.0001) (Figure 2). Dental hygiene students reported significantly more positive attitudes regarding the importance of DVI volunteerism compared to the dental assisting students.

Highest level of understanding of importance for DVI volunteers
DISCUSSION
Mass fatality incidents have benefitted from allied dental professional volunteers as supplemental DVI personnel and there is scant research to demonstrate that allied dental curricula prepares graduates with transferrable skills.18 However, little is known about the knowledge, confidence, and attitudes of allied dental professionals. Current DVI educational assessments lack standardization and little is known about perceptions and the transferability of cognitive, psychomotor, and affective skills, especially for allied dental professionals.2,15-17,29,30 Results from this study revealed statistically significant increases in allied dental professional students perceived DVI knowledge, positive associations between certainty and match accuracy, intra-rater reliability, and positive attitudes for future DVI volunteerism.
Increased confidence and knowledge could help allied dental professionals overcome barriers from seeking specialized training and serving as volunteers. Newcomb et al conducted a similar study which compared low media and multimedia training approaches and reported an increase in scores resulting from the multimedia approach.31 Increases in perceived knowledge from this study and those reported by Newcomb et al.,31 support the recommendations for utilizing multimedia in DVI training.13,31 Results of these studies suggest that incorporation of multimedia learning experiences can provide important foundational knowledge on DVI without posing significant impediments on core curricula.
Participants were asked to indicate their level of certainty regarding accuracy of each match by using two ABFO identification scale terms: “positive” and “possible”. In forensics, these terms are associated with the examiner’s confidence and opinion that their match is correct.27 Prior to data collection for this study, the researchers defined ABFO degrees of certainty for participants during the learning experience and on the post-test survey immediately following the radiographic matches. This controlled for possible confounding issues related to participants’ own interpretation of each term, suggested by Page et al.17 Additionally, the forced binary choice of either “positive” or “possible” allowed for confidence to be assessed without the option of “insufficient information”. The option “insufficient information” would only happen when AM and PM images being compared consist of no common anatomical features (i.e., comparing an anterior periapical radiograph to a molar bitewing radiograph),17 which was not a part of the study design.
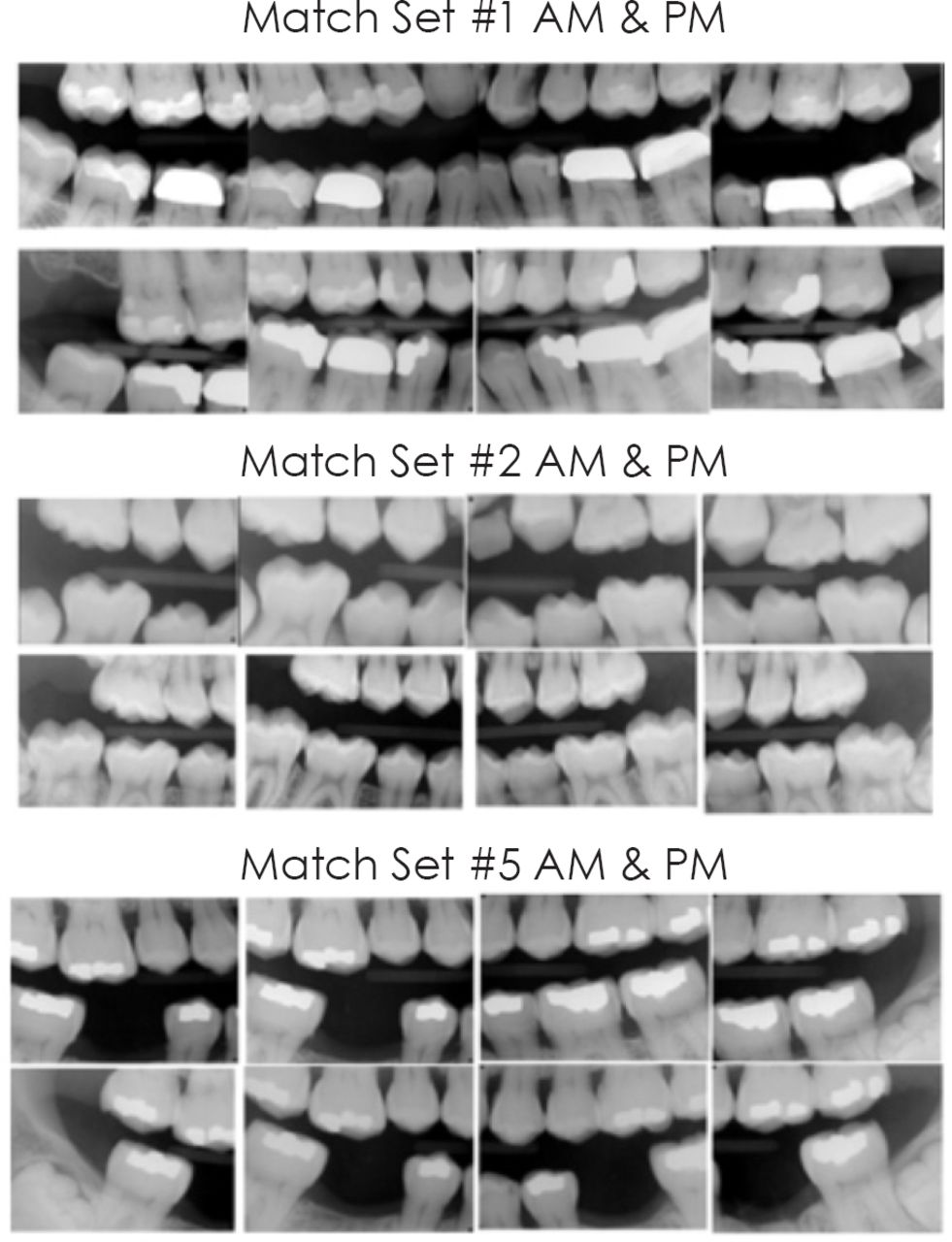
Considering participants demonstrated a statistically significant correlation of their confidence with correct matches, it is unlikely their answers were simple guesses. Since radiographic sets #1 and #2 had the fewest number of clinically detectable dental identifiers (CDDI) to facilitate comparisons, participants were least confident with these match sets. However, participants had an increased certainty of their matches for radiographic set #5, even though it was considered to have few CDDI, but had unique morphological concordant points which visually set it apart from the other match sets. These unique features can be seen in Figure 3 and may explain the level of confidence despite the challenge of the presented cases. Bradshaw et al. reported that participants successfully demonstrated the transferrable skill of reconciling AM radiographs to PM odontograms similar to how participants in the current study demonstrated the transferrable skill of reconciling AM and PM radiographs.18 These findings are also align with Pinchi et al. who included dental students for a study of radiographic match accuracy and reported their rates of accuracy as similar to professionals with forensic odontology training.30 It should be noted, the current study did not attempt to account for possible cognitive bias among the participants, but bias is a concern for DVI volunteers, especially those who have not completed forensic odontology educational programs.

Radiographic match sets
Results from this study showed that the majority (96%) of participants had a moderately or extremely positive affective attitude regarding the importance of volunteerism in DVI following the learning experience. Similarly, a 2014 survey of 334 dental hygienists in the United States showed 85.6% were interested in DVI volunteerism and 91.6% indicated intentions of becoming more involved.32 The current study showed that 77% of the dental hygiene students perceived the importance of volunteerism to be extremely important compared to only 50% of dental assistant students. It is unclear why there was a difference in participants’ perceived value of DVI volunteerism among the two disciplines. Overall results from this study and the findings by Bradshaw et al., show that willingness exists among dental hygienists and dental assistants to volunteer with DVI and if provided with specialized training, they are likely to increase the overall success of DVI teams.32
According to Page et al, differences in accuracy among participants is an indication of individual proficiency.17 Therefore, it is interesting that the dental assistant students performed with lower accuracy rates and less overall confidence, however these participants reported that a previous education presentation on forensics helped them feel more confident when deciding on radiographic matches. This may be explained by differences between the educational experiences of dental hygiene and dental assisting students that include the program length, and rigor of curriculum.
Results from this study suggest that dental hygiene and dental assisting students have foundational skills applicable to successful DVI outcomes and their perceptions and attitudes may be enhanced with additional DVI training, including simple interventions such as a multimedia learning experience. It should be noted that the multimedia learning experience was not overly sophisticated in design and development did not require a significant amount of time or financial investment. Additionally, the learning experience could be offered multiple times for volunteers to review, which is recommended for forensic training.13,14
The ABFO’s degree of certainty is frequently utilized often in DVI, but there is little found in the literature discussing the reliability of using this method for identification purposes. Results from this study identified a positive association between confidence in the participant’s match choice and the accuracy of the match. Several factors may attribute to case difficulty such as quality of radiographs, angulation techniques of the radiographer, and similar CDDI.27 Future research is necessary to determine the overall confidence levels of dental professionals when performing DVI comparison and the relationship to overall accuracy, as well as factors that may be contributing to lower confidence ratings. Results from this study also identified a positive correlation for intra-rater reliability suggesting that each participant consistently performed successfully when deciding on matches.
Limitations of this study may affect internal and external validity of the findings. The small convenience sample may not be representative of other allied dental students or licensed practitioners. Variations in the number of students between academic disciplines created challenges for statistical testing, however, the authors chose comparison tests for unequal sample sizes. The learning experience was not designed as a full curriculum approach and did not test long-term knowledge retention. The PM images of this study were static and did not allow for re-takes, which is often possible in real casework for the purpose of increasing image quality. Additionally, participants completed the study individually and were not able to consult with another person which differs from traditional DVI practice where multiple team members are involved.
CONCLUSION
Allied dental professionals have experience assisting with forensic odontology tasks during MFIs and have aided in successful DVI outcomes. Dental hygiene and dental assisting student participants reported significant improvements of self-perceived knowledge, confidence and attitudes regarding DVI topics and skills. These characteristics may encourage future allied dental professionals to pursue further DVI education opportunities and volunteer service when support is needed for MFIs. Future research is necessary to assess the best practices and modes of DVI training for allied dental professionals that build on existing foundational skills and knowledge.
DISCLOSURES
The authors have no conflicts of interest to disclose. No funding sources were utilized for this research.
Footnotes
NDHRA priority area, Professional development: Education (evaluation).
- Received October 11, 2023.
- Accepted February 21, 2024.
- Copyright © 2024 The American Dental Hygienists’ Association





{kind=link}
{kind=link}
{kind=link}