



Abstract
This case report describes the implementation approach and evaluation of a medical-dental integration (MDI) project in Colorado that embedded dental hygienists (DHs) into 10 medical practice settings. Through the MDI Learning Collaborative, DHs were integrated into primary care medical care practices to provide full-scope dental hygiene care to patients. Dental hygienists were trained to collect quality-improvement metrics on all encounters, including untreated tooth decay, and referred patients with restorative needs to partnering dentists. Cross-sectional, aggregated clinic-level oral health metrics were submitted monthly from 2019-2022. Descriptive statistics were used to describe the population receiving MDI care and interviews were conducted with MDI staff to describe their perspectives on this approach to comprehensive care. A logistic regression model, adjusted for time and practice, compared untreated dental caries in established vs new MDI patient-visits. From 2019-2021, integrated DHs completed 13,458 visits to low-income patients, Medicaid (70%, n=9,421), uninsured (24%, n=3,230), SCHIP (3%, n=404), private (3%, n=404), of various ages: 0-5 (29%, n=3,838), 6-18 (17%, n=2,266), 18-64 (51%, n=6,825), >65 (4%, n=529). A total of 912 visits were provided to pregnant patients. Services included caries risk assessment (n=9,329), fluoride varnish (n=6,722), dental sealants (n=1,391), silver diamine fluoride (n=382), x-rays (n=5,465) and scaling/root-planing (n=2,882). Improvement was found in untreated decay of established vs. new patient-visits in four of the practices. Dental hygienists integrated into medical teams provided full-scope dental hygiene care to patients and expanded access to dental services. Medical-dental integration (MDI) care was variably associated with reduction in untreated decay. Integrating dental hygienists into primary care medical practices has potential to improve oral health-related outcomes, however access to restorative dental care remains a challenge.
INTRODUCTION
In 2000, the first-ever United States (US) Surgeon General’s Report on Oral Health stated that “oral health is more than healthy teeth and is integral to the general health and well-being of all Americans.”1 Twenty years later, the US Surgeon General’s Report: Oral Health in America further emphasized that “the mouth reflects general health and well-being” and that “oral diseases and conditions are associated with other health problems.”2 The most recent report further emphasizes the need to “build an effective health infrastructure that meets the oral health needs of all Americans and integrates oral health effectively into overall health” and “remove known barriers between people and oral health services.”2 Integrating dental hygienists into medical care teams is an emerging approach that has the potential to help build and support the US Surgeon General’s health infrastructure framework. The Delta Dental of Colorado Foundation (DDCOF) has been a leader in testing the integration of dental hygienists into medical practices for the past 14 years. Over the duration of three medical-dental integration projects funded by DDCOF, a total of 43 dental hygienists (DHs) have been integrated into 33 medical practices in 27 healthcare organizations across the state of Colorado. This case report describes the implementation approach and evaluation of a medical-dental integration (MDI) project in Colorado that embedded DHs into ten medical practices.
MEDICAL DENTAL INTEGRATION APPROACH
An MDI Learning Collaborative, led by an implementation team comprised of subject matter experts and the foundation staff, supported practice transformation coaches and practice teams through a quality improvement approach that utilized the MDI Change Package and its drivers (Figure 1). The MDI Change Package was developed from the evaluation of the Co-Location of Dental Hygienist into Medical Practices Project (2008-2011)3 and the Colorado Medical Integration Project (2015-2019).4,5 The MDI Change Package drivers included the following components: engaged leaders, engaged providers/staff, right dental hygienist, devoted time, dental hygienist member of care team, team-based care strategies, and data-driven quality improvement (Figure 2).5 More specifically, the “right dental hygienist” describes someone who is able to work independently yet also builds interprofessional relationships, is a problem-solver who can support building the MDI workflows and processes, and is adaptable to meet the individual needs of the patients. In early 2018, 15 medical practices applied to participate in the project and completed readiness and capacity-to-participate assessments; ten practices were selected to participate based on the assessment findings.

Medical Dental Integration Implementation Approach

Medical Dental Integration Change Package
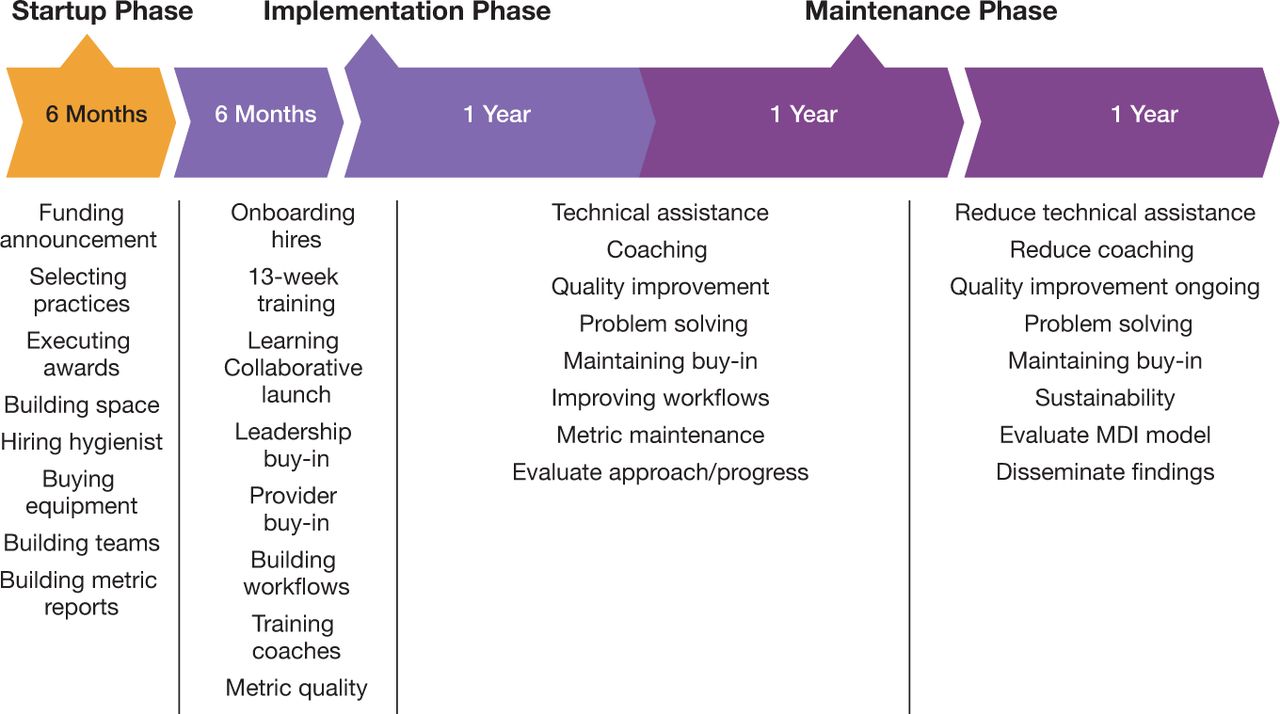
IMPLEMENTATION PHASE I
The MDI Learning Collaborative, supported by the DDCOF, was launched in May 2018. Medical practices were provided technical support for hiring and/or on-boarding their DH staff and building their MDI space within the medical setting. Hiring the right hygienist for the MDI model (a MDI Change Package driver) was emphasized, as was full scope of practice dental hygiene care. The DDCOF provided funds to support the salary of the embedded DH (~$100,000/practice) and DH equipment (~$45,000/practice). The MDI implementation team trained practice transformation coaches from the Colorado primary care organization and a regional health information organization on the necessary oral health knowledge needed to support MDI practices. The evaluation team also trained practices on the collection of oral health metrics and calibrated the integrated DHs on measurement of dental caries.
IMPLEMENTATION PHASE II
Practice transformation coaches began working their medical practices in 2018 through 2019. Each coach supported one to two practices and met with their respective MDI teams monthly. Transformation coaches were supported by implementation team (subject matter experts and foundation staff) throughout the implementation phase. Teams and leaders from the ten participating practices came together in-person every six months to share best practices, lessons-learned, and gain needed skills and knowledge to implement their MDI model. Intensive practice transformation coaching was provided through spring 2020 using MDI quality improvement evaluation metrics. Practice transformation coaching’ support was reduced beginning in spring 2020 as the MDI practices entered the maintenance phase of the project. The evaluation team administered a post-implementation survey in spring 2020 to assess the level-of-integration and achievement of the MDI Change Package drivers; these results informed the level and type of support practices needed as they transitioned into the maintenance phase of the project.
MAINTENANCE PHASE
From spring 2020 through spring 2022, practices were supported by the MDI implementation team with quarterly reviews of the quality improvement metrics and targeted coaching to assist in full attainment of the integration. The COVID-19 pandemic impacted Colorado beginning in March 2020; two participating practices dropped out of the project due to loss of DH staff, lack of patient visits, and shifting priorities related to providing safe care through the pandemic.
EVALUATION PHASE
Metrics
Quality metrics that included monthly processes (dental procedures; count) and outcome (untreated dental disease; yes/no) were collected by the evaluation team from each participating practice throughout project’s adoption, implementation, and maintenance through March 2022. A data dictionary with detailed definitions for each metric was developed using existing dental procedure codes whenever possible and smart codes as needed. Each practice team was trained on metric definitions and provided support on developing a data-collection process and re-trained with team-member turnover. A member of each practice submitted deidentified, aggregated, monthly metrics through an online database program (REDCap©). The evaluation team conducted a quality check of each month’s metrics and reconciled any data discrepancies whenever possible.
Medical Practice Staff Interviews
Interviews with medical practice staff were completed at the conclusion of the MDI project. The overarching goal of the interviews was to assess team members’ perspectives and experiences with this MDI approach including their successes and challenges to maintaining the model of integrated care. Evaluation staff invited practice staff from eight of the participating practices to complete a semi-structured interview in March 2022. Two practices had left the project because of the COVID-19 pandemic, resulting in no remaining team members to interview. Staff were selected based on those who were providing direct patient care and clinic leaders who made administrative decisions for their organizations. Each staff member received up to four email-invitations to participate. One qualitative expert conducted all interviews. A semi-structured interview guide was used to explore perspectives and experiences related to MDI care. All interviews were audio-recorded and professionally transcribed verbatim in a secure system. The evaluation staff utilized content analysis to identify themes and subthemes within and across all interviews. Deductive and inductive approaches were applied from data collected throughout the analysis. Trained qualitative data analysts iteratively read the transcripts, independently coded three documents to develop the coding approach and refine the code book and then met to discuss emergent themes. Once immersion of ideas was reached and a codebook was created, one data-analyst then coded all remaining transcriptions. Open and axial coding of transcripts was used to form the basis of analysis of interview data (ATLAS.ti 7.0, Scientific Software Development GmbH, Berlin, DE).
Data Analysis
The evaluation included an assessment of patients’ oral health as a result of dental hygiene integration. To assess the integration, it was hypothesized that untreated dental caries in established DH patients would be lower than in new patients. It was assumed that new patients who had never received MDI care had not yet been exposed to the integrated MDI care and related restorative services for untreated decay. To test this hypothesis, a multivariate linear regression was used to test whether a higher monthly proportion of established patients seen at each practice was associated with a lower monthly rate of untreated dental caries at the specific practice. Monthly proportions of untreated caries in established-patient care visits were compared to proportions in new-patient visits, adjusting for time and practice. Comparisons were made based on individual medical practice data (rather than aggregated), recognizing that the practices were not comparable enough to generalize the findings. Results from the two practices that withdrew from the project due to the COVID pandemic were not included. Results were converted to percentages for reporting purposes.
RESULTS
Between September 1, 2018 and March 31, 2022, participating practices provided 13,458 dental hygiene visits across 30 counties in Colorado. Dental hygienists provided full-scope dental hygiene care to a broad age range of patients aged 0-5 years (29%, n=3,838), 6-18 years (17%, n=2,266), 18-64 years (51%, n=6,825), >65 years (4%, n=529). A total of 912 of the integrated visits were to pregnant people. Most patients were insured by Medicaid (70%, n=9,421). Dental hygienists provided full-scope of practice dental hygiene care including caries risk assessment (9,329), fluoride varnish applications (6,722), x-rays (5,465), oral prophylaxis (5,161), scaling and root planing (2,882), dental sealants (1,391), and silver diamine fluoride treatments (382). Across all participating practices, during 36 of the 42 months of the project, integrated dental hygienists provided dental sealants to over 75% of eligible patients (6-9 years).
The evaluation team completed 19 interviews with MDI team members from eight of the original ten participating practices at the end of the maintenance phase of the project. In general, team members were overwhelmingly enthusiastic about this MDI model. Themes that emerged regarding the project successes included that MDI: expanded access to preventive and restorative dental services, leveraged medical visits for dental care, and promoted awareness that oral health is part of overall health. While barriers to the approach were mentioned by participants, no major themes emerged in this area; minor themes were related to challenges with financial solvency such as lack of sufficient patients (especially in small clinics) and lack of insurance reimbursement (e.g., uninsured patients). Those interviewed expressed successes driving financially sustainable programs including serving insured patients (e.g., Medicaid) and having a sufficient patient volume. Challenges to the financial sustainability of the MDI model centered largely around not receiving reimbursement for care rendered. Major and minor interview themes are shown in Table I.
Medical Practice Staff Perspectives Regarding Integrated Dental Hygiene (n=18)
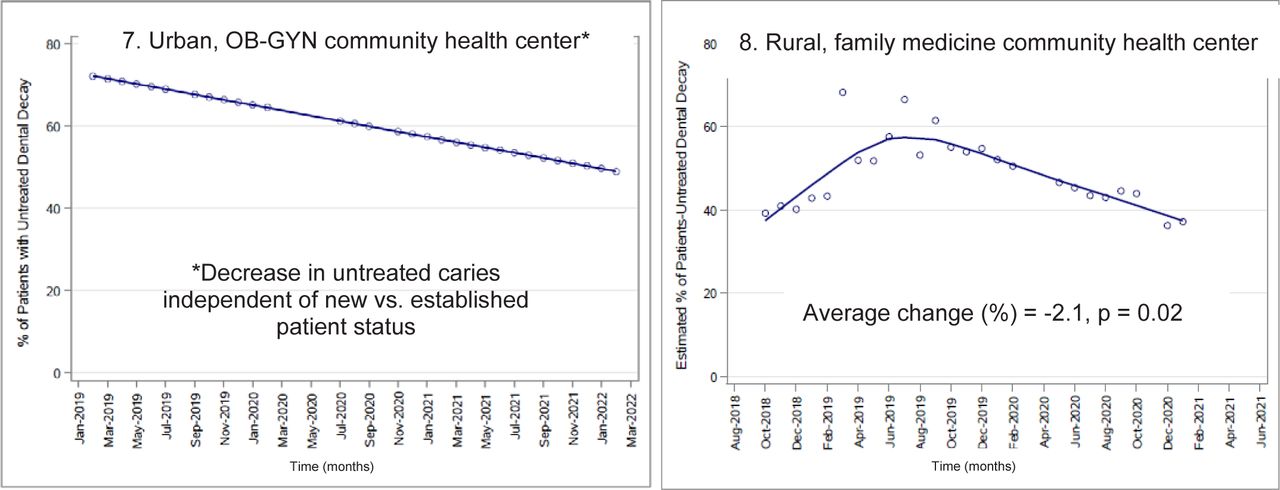
In a multivariate linear regression adjusting for time and medical practice, the proportion of established patient-visits vs. new patient-visits with untreated caries significantly declined in two practices (one urban pediatric and one rural family medicine community health center) (Figure 3.). There was a nearly significant decline in untreated caries in two small family medicine community health centers. In two practices, there was a substantial decrease in the proportion of patient visits with untreated caries, independent of being an established vs new patient.


Adjusted logistic regression analysis comparing change in proportion patients with untreated dental caries in established patients vs. new patients of dental hygienists; adjusted for time and practice.
CONCLUSION
This case report describes an approach to implementing an MDI model that includes the use of a learning collaborative comprised of subject matter experts and an implementation team to support practice transformation coaches and practice teams with the MDI Change Package and builds upon previous work regarding the feasibility and implementation of this MDI model. The evaluation of this approach suggests that integrating dental hygienists into medical practices expands access to dental care for both children and adults and has potential to improve their oral health. Medical dental integration is beginning to expand across the country and is a realistic mechanism to support the US Surgeon General’s Framework for Action by incorporating oral health into overall health and removing known barriers between people and oral health services. Integrating dental hygienists into medical practices has the potential to expand access to oral health care in marginalized populations and promote health equity.
ACKNOWLEDGEMENTS
Thanks are extended to Mirella Chavez, Allison Cusick, Megan Wilson, Monica Woods, and the Delta Dental of Colorado Foundation staff for their partnership in the MDI project.
Footnotes
NDHRA priority area, Population level: Access to care (interventions).
DISCLOSURE
Delta Dental of Colorado Foundation funded the implementation and evaluation of the Colorado Medical Dental Integration Project.
- Received April 26, 2023.
- Accepted May 19, 2023.
- Copyright © 2023 The American Dental Hygienists’ Association





{kind=link}
{kind=link}
{kind=link}
{kind=link}