



Abstract
The American Dental Hygienists’ Association (ADHA) defines direct access as the ability of a dental hygienist to initiate treatment based on their assessment of patient’s needs without the specific authorization of a dentist, treat the patient without the physical presence of a dentist, and maintain a provider-patient relationship. In 2000 there were nine direct access states; currently there are 42 states that have authorized some form of direct access. The ADHA has been instrumental in these legislative initiatives through strong advocacy efforts. While research and data support the benefits of direct preventive/therapeutic care provided by dental hygienists, many barriers remain. This paper chronicles key partnerships which have influenced and advocated for direct access and the recognition of dental hygienists as primary health care providers. The National Governors Association (NGA) released a report in 2014 suggesting that dental hygienists be “deployed” outside of dental offices as one strategy to increase access to oral health care along with reducing restrictive dental practice acts and increasing the scope of practice for dental hygienists. The December 2021 release of the National Institutes of Health report, Oral Health in America, further supports greater access to dental hygiene preventive/therapeutic care. This paper also reflects on opportunities and barriers as they relate to workforce policy, provides examples of effective state policies, and illustrates an educational curriculum specifically created to prepare dental hygienists to provide oral health services in settings outside of the dental office. Dental hygiene education must ensure that graduates are future-ready as essential health care providers, prepared to deliver direct access to dental hygiene care.
INTRODUCTION
In celebration of the 100th anniversary of the American Dental Hygienists’ Association (ADHA) this paper will provide an overview (past, present, future) of the practice of dental hygiene in the United States (US) as it relates to consumers’ direct access to preventive/therapeutic care provided by the dental hygienist. It will highlight the supportive role that the ADHA and its state associations have played in supporting access to care for all populations. Dental hygiene was conceived on the concepts of disease prevention and oral health promotion. In 1913, Dr. Alfred Civilion Fones opened the first dental hygiene program.1 Since its inception, the profession has been based on oral hygiene, oral health education, and preventive oral health care services. Today, the profession continues to build on this foundation of the promotion of health and wellness, particularly as oral health has been shown to be integral to overall health. While the dental hygiene profession began in 1913, the ADHA was established in 1923 and now in 2023 celebrates its centennial. The current mission of the ADHA is to “advance the art and science of dental hygiene by ensuring access to quality oral health care, increasing awareness of the cost-effective benefits of prevention, promoting the highest standards of dental hygiene education, licensure, practice and research, and representing and promoting the interests of dental hygienists.”2 The ADHA represents the interests of over 226,000 registered dental hygienists in the US.
Direct Access to Dental Hygiene Services
One of the highest priorities of the ADHA is increasing access to oral health care for all populations across the lifespan. Direct access has been defined as “the ability of a dental hygienist to initiate treatment based on their assessment of patient’s needs without the specific authorization of a dentist, treat the patient without the presence of a dentist, and maintain a provider-patient relationship.”3 The US Surgeon General’s report on oral health in 2000 was a seminal moment and arguably for the first time brought oral health to the forefront of the nation’s overall health. The report issued in 2000 highlighted lack of access to oral health care as a critical issue in the US due to disparities in the health care delivery system.4 The role of the dental hygienists was largely absent in addressing inequities and disparities in oral health care in the Surgeon General’s Report. In 2014, the National Governors Association (NGA) released a paper on the role of dental hygienists in providing access to oral health care.5 The NGA acknowledged that oral health is an important determinant of overall health, and that dental disease and poor oral health are preventable when individuals have regular access to oral health care and patient education. The NGA recognized the need for expanding the oral health care workforce and advanced the idea of dental hygienists providing care beyond brick-and-mortar dental offices to reach those individuals who were not currently receiving oral health care services. Further consideration around supervision laws that created barriers for individuals to access dental hygiene oral health care services, as well as revision of reimbursement rules were key strategies recommended by the NGA. With the NGA fully on board regarding the profession’s role in providing increased access to oral health care, the ADHA was at work at the national level to upgrade dental hygiene’s occupational classification.
Occupational Classification and Advancing the Profession
The ADHA engaged in a multi-year advocacy effort aimed at seeking changes to the US Bureau of Labor Statistics Standard Occupational Classification (SOC) to more accurately reflect the practice of dental hygiene. The SOC is a classification system used by federal statistical agencies to “classify workers into occupational categories for the purpose of collecting, calculating, or disseminating data.”6 Occupational classification information such as employment levels and projections, pay and benefits, skills required, and other demographics are widely used by the public, interested stakeholders and public policymakers. As a result of ADHA’s efforts, a substantive revision in dental hygiene’s classification was approved. Dental hygienists had been classified in 2014 by the SOC as “Health Technologists and Technicians,” however the ADHA recommended that this be changed to “Health Diagnosing and Treating Practitioners,” the same grouping as dentists. Those advocacy efforts proved to be successful and as of 2018 the SOC classifies dental hygienists as “Healthcare Diagnosing and Treating Practitioners”. The full SOC description for dental hygiene is as follows:
“Administer oral hygiene care to patients. Assess patient oral hygiene problems or needs and maintain health records. Advise patients on oral health maintenance and disease prevention. May provide advanced care such as providing fluoride treatment or administering topical anesthesia.”
This revised classification represents a significant advancement, especially considering that a dental hygiene diagnosis requires evidence-based critical analysis and interpretation of assessments to reach conclusions about the patient’s dental hygiene treatment needs. Dental hygienists are educated and licensed to provide their patients with a dental hygiene diagnosis, as part of the dental hygiene process of care. The dental hygiene process of care can be found in the ADHA Standards for Clinical Dental Hygiene Practice.7
In 2021 the National Institutes of Health (NIH) released the Oral Health in America: Opportunities and Challenges report.8 While dental hygiene was minimally recognized in the 2000 Surgeon General Report, the 2021 Oral Health report fully engaged the profession. The ADHA was invited to participate in the development of the report with the Chief Executive Officer, Ann Battrell, MSDH, FADHA serving as a scientific reviewer. Fourteen dental hygienists working in a variety of settings (education, government, professional organizations, public health, research) also served as contributing authors. Using the Surgeon General report from 2000 as a baseline on the status of oral health in America, the 2021 NIH report highlighted areas of improvement over the two-decade time period and identified continuing challenges that remained unaddressed. For example, the number of individuals receiving oral health services at Federally Qualified Health Centers (FQHCs) across the US increased from 1.4 million in 2001 to nearly 5.2 million in 2020. While preschoolers experienced the most substantial decline in untreated dental caries (19% in 2000, 10% in 2021), working-age adults and older adults still faced increased disparities and lack of access to oral health care. Dental hygienists were referenced seventy-five times in the report, citing the essential roles they have played in addressing unmet oral health care needs. The importance of the inclusion of dental hygienists in non-traditional settings for reaching persons unable to access private or public dental settings, such as the homebound, institutionalized, and those who lack transportation, was highlighted in the report.
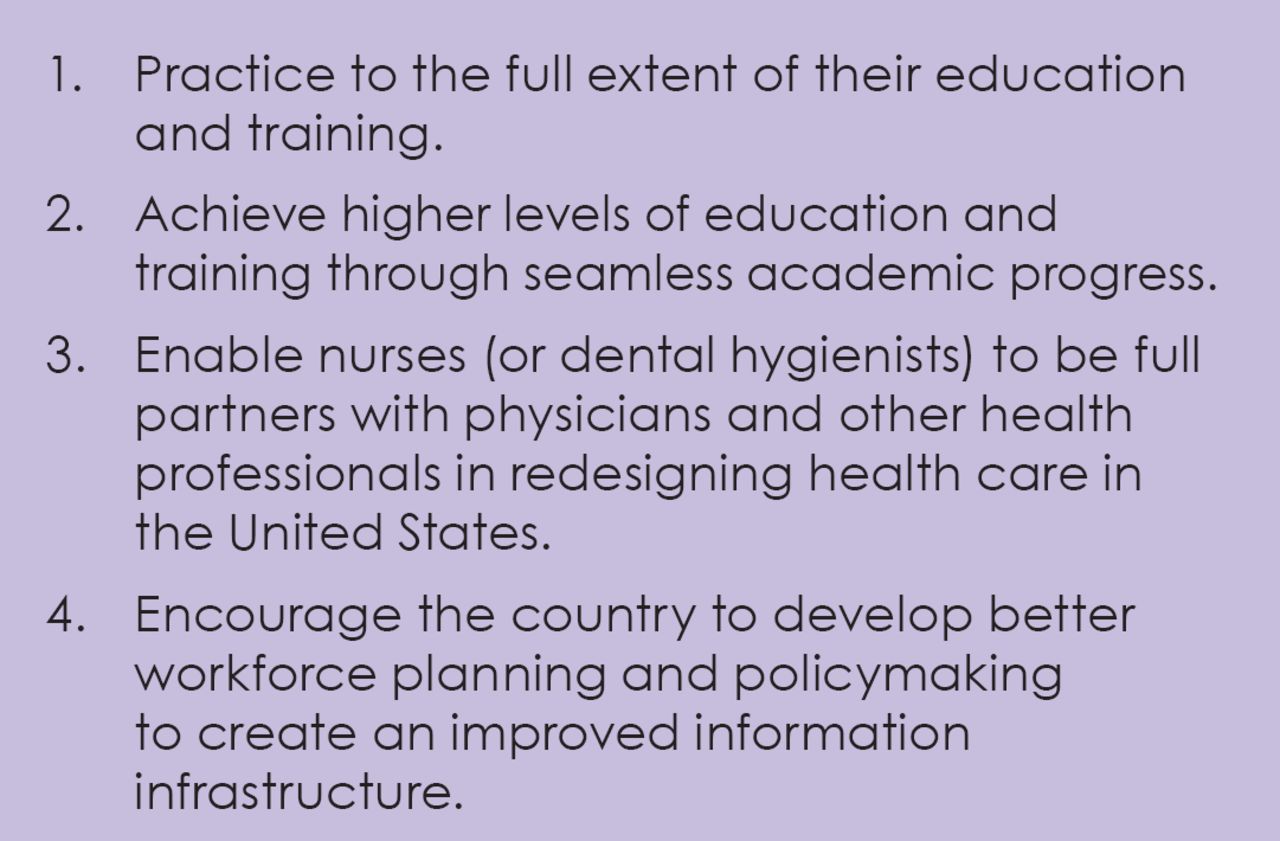
Many state dental practice acts continue to present barriers to dental hygienists providing care in non-traditional settings. The 2021 report acknowledges the importance of dental practice acts that allow for direct access to dental hygienists. Examples of dental hygienists in medical-dental integration settings, such as pediatric offices, community healthcare and safety net practices, are highlighted as important methods for increasing access to oral health care. Restrictive dental practice acts not only limit the practice of dental hygiene, but they also serve to restrict educational programs. The roles educational programs can take in the development of improved workforce models are limited by state dental practice acts that restrict dental hygienists from providing the full range of services for which they are educated. One barrier currently faced by dental hygienists is that only nineteen states (38%) allow dental hygienists to independently bill Medicaid for oral health services.9 Section 4 of the Oral Health in America report notes that the challenges facing better integration of dental hygienists into oral health care mirror similar problems faced by advanced practitioners in the nursing profession.8 As dental hygienists transition to providing care in non-traditional settings, there is much to be learned from the challenges and solutions created by the nursing profession (Figure 1).10

Key messages from the nursing profession regarding advocacy strategies for becoming integrated partners and leaders in health care8
At the time of the Surgeon General’s Report in 2000 there were only nine states that allowed direct access to dental hygiene preventive/therapeutic oral health care services. By the time the Oral Health in America Report was released in 2021, there were forty-two states that allowed for direct access to oral health care provided by a dental hygienist. While there has been a significant increase in direct access states, a review of the individual state practice acts reveals a wide range of discrepancies regarding the specifics of what direct access entails on a state by state basis.
Direct Access: Opportunities and Barriers
A review of the progression of direct access shows that eight states (Washington [1984], Colorado [1987], New Hampshire [1993], Oregon [1997], California [1998], Nevada [1998], Connecticut [1999], New Mexico [1999]) allowed for some sort of direct access to dental hygienists at the time of the Surgeon General’s 2000 report. Since that time, direct access gradually progressed to 28 states in 2008, 34 states in 2011, and finally 42 states in 2021.3 The remaining eight states that do not allow any form of direct access to dental hygiene oral health care services includes Alabama, Delaware, Hawaii, Louisiana, Mississippi, North Carolina, North Dakota, and New Jersey.3
The Commission on Dental Accreditation (CODA) has established national accreditation standards for dental hygiene education programs which are uniform across the US.11 As a result, of these universal standards, there should be little variability when it comes to the practice of dental hygiene as it applies to direct access. Yet there is widespread variation in patient participation eligibility, extent of dentist supervision, allowed work settings, licensure requirements, reimbursement practices, and the overall effectiveness of policy implementation.3 These variations have been shown to significantly impact the ability of patients to have direct access to dental hygienists in non-traditional settings.12
Shortly after the release of the Report of the Surgeon General in 2000, the ADHA began a collaboration with the Oral Health Workforce Research Center at the Center for Health Workforce Studies in the School of Public Health at the University of Albany to construct the Dental Hygiene Professional Practice Index (DHPPI). The DHPPI was designed to numerically score statutes and regulations governing the legal scope of dental hygiene practice in the US.13 The instrument calculated composite scores ranging from 0 (more restrictive environment) to 100 (less restrictive environment) to quantify regulations, supervision, tasks (procedures) that could be performed, and reimbursement policies to measure the opportunity for dental hygienists to provide oral health services to the full scope of their education and training.13 The DHPPI was then used in 2014 to re-score the scope of dental hygiene practice in each state and report longitudinal changes that took place since 2001.14 In 2016, new variables were added to be more reflective of the full range of dental hygiene practice including public health settings.15 The DHPPI has been used in a variety of research studies examining dental hygienists’ scope of practice as it relates to access to care and oral health outcomes. Wing and Marier used the DHPPI with a large database of dental insurance claims to examine the costs of dental services provided by dentists versus those provided by dental hygienists.16 Findings revealed that task-specific occupational regulations increased costs of care by 12% and that settings allowing for direct reimbursement to dental hygienists by insurers increased the probability of a person having an oral prophylaxis by 4.3%.
Allowing dental hygienists to have direct reimbursement by Medicaid trended in the same direction, increasing the probability of a person receiving a prophylaxis by 3.7%.16 Maxey et al. used the DHPPI and the 2004-2012 UDS (Uniform Data System) to explore how variations in state dental hygienists’ workforce policies influenced the proportion of dental services provided at federally qualified health centers (FQHCs).17 Findings revealed higher DHPPI scores were associated with health centers delivering dental services to a higher proportion of the health center patient population,17 suggesting that dental hygienists’ scope of practice may influence the availability of dental services provided at health centers. Langelier et al. used the DHPPI to score state-level scopes of practice in all fifty states and the District of Columbia in 2001 and 2014.18 They proceeded to analyze the association of each state’s scope of practice score with the oral health outcome of extractions of permanent teeth in older adults.18 Findings revealed more autonomous scopes of practice were significantly associated with fewer extractions of permanent teeth. Akinlotan et al. used the DHPPI in 2022 to examine emergency department visits for non-traumatic dental visits that were preventable in ten states.19 Findings revealed that 23.8% of all non-traumatic emergency department visits were preventable and that restrictive scopes of state dental practice policies were associated with higher numbers of preventable dental emergency department visits.
The DHPPI has also been used to examine the impact of state dental practice acts on the outcomes of school-based oral health programs. In a study by Simmer-Beck et al. the direct access statutes of neighboring states Missouri and Kansas were compared in regards to the oral health outcomes of children enrolled in school-based based programs.20 The DHPPI scores for these states were 63 and 53, respectively.15 Although the scores were comparable, with Missouri having a slightly less restrictive environment per the DHPPI ranking, there were significant differences in how the school-based programs operated. Missouri’s dental practice act allowed for dental hygienists with at a minimum of three years’ experience to provide care without a dentist’s exam only if the child was eligible for Medicaid. This inclusion criteria resulted in concerns from school administrators regarding equitable treatment for all students and was deemed unacceptable for the program. Under the restrictions placed by the statute, the only way to treat all children in a Missouri school-based setting was for a dentist to provide the examination and diagnose the need for preventive services (prophylaxis and sealants) prior to the provision of care by a dental hygienist. Although fully qualified for making a dental hygiene diagnosis as demonstrated by other state statues and the SOC classification of the profession, Missouri dental hygienists were not allowed to diagnose the need for preventive services for children who did not require financial assistance. In stark contrast, the Kansas dental practice act allows for Extended Care Permit (direct access) dental hygienists to deliver care without the direct supervision of a dentist and without financial restrictions in any setting where the individual “lacks access to dental care.”
Collectively, the above research studies16-20 provide strong evidence of positive associations between less restrictive statutes regulating dental hygienists’ scope of practice and direct access with improved patient outcomes. It is also important to note that each study discussed limitations relative to the DHPPI scores reflecting state laws, rather than the implementation. If the DHPPI score reflected implementation of state law, the associations would likely have been even stronger.
This limitation on access to care is most profound when examining scores for direct Medicaid reimbursement to dental hygienists. Currently nineteen states (38%) have statutory or regulatory language allowing for direct reimbursement by Medicaid for services provided by dental hygienists.9 Implementation of this policy has resulted in much disparity across states. For the purposes of this paper, all nineteen states were contacted in an effort to provide readers greater clarity regarding direct Medicaid reimbursement in these states. While all nineteen states reported dental hygienists could be directly reimbursed by Medicaid, the circumstances varied (Table 1). Fifteen of the nineteen states allow dental hygienists to be directly reimbursed by Medicaid without any special license designations or contract with a dentist or group practice. The remaining states commented on the barriers remaining to be overcome before direct reimbursement for dental hygienists could be implemented. For example, several respondents noted that there was much effort involved when working with state Medicaid systems for dental hygienists to be accepted as providers. One state, Missouri, reported a clear process was not in place even though the law was established in 2001. In this instance, the Missouri legislature passed legislation allowing Medicaid “to reimburse any eligible provider who provides fluoride treatments, teeth cleaning and sealants.”21 However, it took Medicaid in Missouri more than two decades to update their computer system to include dental hygienists as “eligible providers” for reimbursement in the state and no dental hygienists in Missouri are collecting Medicaid payment directly to date. As shown in Table I, significant barriers to billing Medicaid include dental hygienists being required to have a special licensure designation, needing a signed agreement or affiliation with a dentist or group accepting Medicaid, and accepting a lower direct reimbursement rate than dentists for the same services.
Summary of state responses related to Medicaid reimbursement for dental hygienists (Spring/Summer 2023)
In 2018 the PEW Charitable Trusts explored policy and regulatory barriers that were impediments to school-based sealant programs.22 State dental directors identified several barriers with two major underlying sources; state dental practice acts that define the scope of practice and supervision requirements for dental hygienists and Medicaid policies prohibiting reimbursement for care provided outside of a dental office or clinic. Regulations and rules are intended to protect the public safety and promote the efficient use of public resources; however, these same policies have impeded these aims even though governmental and health organizations have endorsed school sealant programs for reaching at risk children.
Workforce innovation plays a vital role in providing vulnerable populations fair and just opportunities to access high quality, affordable, culturally appropriate oral health care. In 2018 the US Departments of Health and Human Services, Department of the Treasury, and the Department of Labor, joined forces to present, “Reforming Americas Healthcare System Through Choice and Competition.”12 This document provides recommendations on the removal of unjustified barriers to the delivery of oral health care. More specifically, the report recommends:
States should consider changes to scope-of-practice statues and supervision requirements to allow all health care providers to practice at the top of their license, utilizing their full skill set.
States should consider eliminating requirements for rigid collaborative practice and supervision agreements between physicians and dentists and their care extenders (e.g., physician assistants, dental hygienists) that are not justified by legitimate health and safety concerns.
These barriers have been reiterated by the US Department of Health and Human Services, US Department of the Treasury, and US Department of Labor.12 These governmental organizations universally recommend broadening dental hygienists’ scope of practice when there are no clear risks of consumer safety as a means to increase the supply of providers, increase competition, and reduce costs to the public.12 What appear to be inconsequential limitations to scope of practice can completely prohibit implementing otherwise effective policy. Less restrictive supervision requirements and direct reimbursement are important policy tools that every state should use to increase access and improve oral health outcomes.
In a 2021 study on workforce equity, Mertz et al. explored how rulemaking, oversight, and appropriations have impacted the implementation of oral health care workforce policy.23 Findings revealed incidences where state dental boards intentionally drew out legislative processes and restricted scope of practice, education requirements, and reimbursement processes in order to delay policy implementation.23 Mertz et al. describe how most professions in the US, including dentistry, have maintained a traditional hierarchy, as a result of longstanding racial, sex, and colonial exclusionary practices. The hierarchical design of dental professions includes, hegemonic paternalism, and dentist-led oversight of all dental occupations on workforce equity and consumer protection.23 This can be seen in dentistry by the professions use of states to maintain these hierarchies using public policy (by regulation of allied dental providers, majority female, through boards controlled by dentistry, majority male). Policy advocacy can improve health equity by removing outdated barriers that have not been shown to improve public safety and ultimately restrict access to dental hygiene care.
Direct Access: Successful State Policies
Colorado, one of the early direct access states, provides a good example of how an effective state policy had increased access to oral health services. Over the past 35 years, dental hygienists licensed in Colorado have been able to provide dental hygiene care without authorization or supervision of a dentist and can also own their own practice (legislation enacted in 1987).24 The Colorado Dental Board Practice Act outlines the preventive and therapeutic care provided by unsupervised dental hygienists.25 A few of these services include, providing a dental hygiene assessment, dental hygiene diagnosis, dental hygiene treatment planning, administration of local anesthesia (with permit), scaling and root planning, and prescribing and administering fluoride products. A full list of procedures can be found in the Colorado Dental Practice Act.25 Wisconsin is another example of effective direct access policies. Beginning in 2017, registered dental hygienists can provide services with no further licensure requirements. This legislative change allows for dental hygienists to work in settings such as medical offices, schools, nursing home, and hospitals, resulting in increased access to care for patients of all ages across the state. It is also noteworthy that Oregon and Colorado became the first states, in 2004 and 2009 respectively, to include the dental hygiene diagnosis as part of the dental hygienists’ scope of practice.26 Oregon statute specifically includes diagnosis within the definition of dental hygiene and permits dental hygienists to “diagnose, treatment plan and provide dental hygiene services.” Under Colorado law, “dental hygiene diagnosis” means the identification of existing oral health problem(s) that a dental hygienist is qualified and licensed to treat within the scope of dental hygiene practice. All health care providers, including dental hygienists, need to be able to practice to the fullest extent of their education.
In 2017, at the request of Georgia State Senator Valencia Seay, the US Federal Trade Commission (FTC) staff submitted a letter of comment on a direct access bill.27 The FTC has a dual mission to protect consumers and promote competition and their letter of comment concluded that “fewer restrictions likely would enhance competition in the provision of preventive dental care services and expand access to care, especially for Georgia’s most vulnerable populations.” The FTC has a long history of addressing competition issues in oral health, particularly in the area of overly restrictive supervision and impediments to scope of practice. Given the preventable nature of oral disease, policymakers across the country are urged to take the recommended action to increase access to care and improve the public’s oral and overall health. Efforts on behalf of the dental hygiene profession and the public by professional organizations, such as the ADHA, are ongoing to advocate for increased access to care and improved oral health outcomes for all populations across the lifespan.
Direct Access: Preparing the Future Workforce
Oregon provides an excellent example of how dental hygiene educational programs can prepare graduates to be ready to directly begin practicing in non-traditional settings. In 1997-98, legislation in Oregon established a “limited access” permit for licensed dental hygienists in the state to provide direct access to care.28 The original legislation required 5,000 hours of supervised practice and completion of 40 hours of continuing education for the limited access permit (Pathway #1).28 Informal survey results generated at the conclusion of workshops held for limited access permit holders by the Oregon Dental Hygienists’ Association and Pacific University in 2005-2006, found that participants did not feel requirements for obtaining their limited access permit adequately prepared them to work as direct access providers. Collaboration and advocacy with stakeholders including Oregon dental hygiene program directors, the Oregon Dental and Dental Hygienists’ Associations, the Oregon Board of Dentistry, and the Oregon legislature resulted in a second pathway to obtain a limited access permit directly upon graduation from an accredited, participating dental hygiene program in the state (Pathway #2).
Pathway #2 states that the applicant must complete a course of study approved by the Oregon Board of Dentistry that includes at least 500 hours of dental hygiene practice with “limited access” patients while under the supervision of dental or dental hygiene faculty of an accredited program. This pathway is based on the deliberate actions incorporated into the Pacific University curriculum to ensure students are able to graduate ready to deliver care via direct access. Accreditation by CODA requires that dental hygiene students complete at least 500 hours of supervised clinical practice.11 A majority of these hours are completed in onsite clinics with patients who may also meet the classification of “limited access.” However, at Pacific University, senior dental hygiene students spend approximately 25% of their clinical hours working at off-campus fieldwork sites alongside limited access dental hygienist providers. The combination of on-campus patients and off-campus fieldwork patients meets the legislative requirement of 500 hours of supervised clinical practice with “limited access” patients.
A 2015 study found that the number of limited access dental hygienists in Oregon had increased by over 50% since the implementation of Pathway #2.28 Barriers continue to exist including the challenge of insurance reimbursement, a lack of knowledge regarding how to begin an independent practice, equipment cost and maintenance, and how to establish a patient base. The Pacific University Dental Hygiene Program has implemented curricular changes aimed at reducing the barriers for students graduating from the program. A 2016 study evaluated the impact of expanded practice dental hygienists (EPDH) in Oregon.29 Responding EPDHs reported providing dental hygiene oral healthcare services to populations in a variety of settings, including, residential care facilities, primary and secondar schools, homebound adults, community health clinics, nursing homes, foster homes to name a few. EPDHs were asked to indicate their success in obtaining reimbursement from the Oregon Health Plan or other insurance plans. Thirty-nine percent of those who responded stated that they had never been successful receiving third party reimbursement. Further research is needed to examine the impact of these graduates on access to oral healthcare.
In the 2015 ADHA report, Transforming Dental Hygiene Education and Profession for the 21st Century, it was noted that the “dental hygiene curriculum must change to provide dental hygienists with the requisite education necessary to serve in instrumental roles that address the oral health of diverse populations and also contribute to improved access to care.”30 There is much to be learned from the experiences of collaboration and advocacy undertaken by Pacific University and the partnerships that were formed for legislative change in Oregon. Educating all stakeholders about the impact of less restrictive licensure policies that result in increased access to care through direct access to the preventive and therapeutic care of dental hygienists can go a long way toward meeting the oral health care needs of all.
CONCLUSION
Momentum has been building during the 21st century in the advancements made to increase access to dental hygiene care in the US. Seminal papers and reports have provided a strong foundation of research and evidence to support greater access to dental hygiene preventive/therapeutic care through direct access.
Recommendations aimed at further increasing direct access to dental hygiene care include:
Revising state practice acts to enable dental hygienists to practice to the full extent of their education and training.
Developing workforce models culminating in:
Graduation from an accredited institution
Professional licensure
Direct access to dental hygiene preventive/therapeutic care
Conducting research aimed at documenting outcomes around greater access to dental hygiene care.
While there has been good progress over the course of the past two decades, much remains to be done to truly achieve the goal of patients across the US having direct access to dental hygiene preventive/therapeutic care. The ADHA has remained a strong force in this effort, but it will take the resolve of all dental hygienists and advocates for direct access for it to become a standard across all states.
Footnotes
NDHRA priority area: Professional development: Regulation (emerging workforce models)
DISCLOSURES
The authors have no conflicts of interest to disclose. No outside funding was received for this paper.
- Received July 24, 2023.
- Accepted September 18, 2023.
- Copyright © 2023 The American Dental Hygienists’ Association





{kind=link}