



Abstract
Purpose: Human papillomavirus (HPV), a sexually transmitted virus that has been identified in over two-thirds of all oropharyngeal cancers. Oral health care professionals play a key role in educating the public regarding HPV and the role of vaccinations. The purpose of this study was to examine dental hygiene and dental therapy students’ perceptions of the importance of and their confidence with applying brief motivational interviewing (BMI) during patient counseling regarding the human papilloma virus (HPV).
Methods: A convenience sample of dental hygiene and dual degree dental hygiene/dental therapy students (n=32) participated in an enhanced BMI curriculum that included a 90-minute HPV BMI coaching and role-playing session on the use of eight MI strategies and the technique of elicit-provide-elicit. Questionnaires assessing participants’ perceptions were disseminated at three time points; prior to the HPV BMI training (pre-test), immediately after the coaching and role-playing session (post-test 1) and after the participants had applied their HPV BMI skills during two patient interactions that included self-assessment and faculty feedback (post-test 2).
Results: All the students in the sample (n=32) completed the three questionnaires. While participants’ perception of the importance of BMI increased for three of the eight strategies (pre-test to post-test 2), it was not statistically significant. Perceptions of confidence in applying of BMI increased for seven of the strategies (pre-test to post-test 1). Statistical significance was achieved for the “Use of the Importance Ruler” strategy (p=0.003) from pretest to posttest 1 and pre-test to post-test 2 (p=0.003).
Conclusion: Results indicate that an enhanced HPV BMI coaching curriculum in addition and two HPV BMI sessions with patients is not enough training to retain confidence overtime. Future research should investigate strategies, such as additional coaching and role-playing sessions, for retaining confidence with applying BMI for HPV discussions during patient care.
- motivational interviewing
- brief motivational interviewing
- dental hygiene students
- dental therapy students
- patient education
- HPV education
- oropharyngeal cancer
Introduction
Oral health care professionals play a key role in the prevention and reduction of the incidence of oropharyngeal cancer (OPC).1 Concurrently, the human papillomavirus (HPV) is the most common sexually transmitted infection (STI), and has been identified in 70% of all OPC.2 Vaccines for the HPV first became available in 2006 and Healthy People 2020 set the HPV vaccine uptake goal in the United States (US) at 80%, yet vaccine acceptance is well below this threshold.3
However, HPV infection is a sensitive topic and oral health care professionals have reported ethical dilemmas on whether HPV related topics should be addressed in the dental office or by a medical provider.4–6 Thompson et al. reported while dental hygienists view their role as prevention specialists in the reduction of HPV positive OPCs, they lack the training and resources for discussing HPV related topics.7 Additionally, prior research has shown that health care providers lack communication skills and confidence discussing HPV related topics during patient care.4,6,8–10 Despite these noted barriers, Stull et al. 2020 found that parents of adolescents are comfortable having HPV related discussions with their dentists and dental hygienists and expect these oral health care professionals to provide HPV counseling.11
Motivational Interviewing (MI) is evidence-based patient-centered counselling to support a positive behavior change.12 Recent studies have explored MI as a communication intervention for HPV related topics during patient care.10,13 In a randomized clinical trial of medical professionals (n=188) a range of interventions including parent education on HPV, vaccine fact sheet, and MI communication training were studied.14 Dempsey et al. found the HPV fact sheet and MI were most frequency used among medical professional with the majority (91%) of the participants reporting that they were most likely to use MI as the preferred communication for HPV-related topics.14
Motivational interviewing encompasses four components: 1) collaboration, 2) acceptance, 3) compassion, and 4) evocation, aimed at supporting patient autonomy, referred to as the “spirit of MI”12,15 Motivational interviewing allows providers to “roll with resistance” to avoid conflict during patient-provider communication.16 Additionally, MI supports self-efficacy to build patient’s confidence in the behavior change process.12 Utilizing all four components or the “spirit of MI” has been shown to build trust and rapport between both the patient and the provider.12,16
Guiding strategies are used within the MI process to support behavior change. These strategies include open-ended questions that allow the patient an opportunity to craft a response to provide insight on their perceptions; affirmations to encourage the patient’s strengths; reflections to allow the provider to demonstrate an understanding of the patient’s perceptions, ambivalence, and efforts; and summaries to close the MI session.12,16 In a study of health care providers’ communication regarding HPV vaccinations for adolescents, Reno et al. found the guiding strategies of affirmations and reflections were used more than 75% of the time.10 There are additional “RULEs” to follow to align with the spirit of MI. Resist the righting reflex (R), means providers do not “fix” or “change” the patient’s health behaviors.12,16 Understanding (U) is the demonstration of empathy for the patient’s motivations and perceptions of change.12,16 Listening (L) with empathy is the provider’s compassion for the patient.12,16 Empower (E) is to support patient autonomy and build the patient’s own self-efficacy for change.12,16
Motivational interviewing as a communication strategy for positive oral health behavior change has been used in dental hygiene education for nearly a decade.17–20 An early study by Croffoot et al. identified the inclusion of MI in the dental hygiene curriculum improved students’ use of open questions and reflections.17 In another study Curry et al. reported dental hygiene alumni valued their MI training during their education and identified MI as a superior communication approach.21 However, multiple studies have identified time constraints during a dental appointment as a barrier using MI.19–21 Therefore, brief motivational interviewing (BMI), a derivative of MI, is ideal for health care professionals with limited time (5-10 minutes) to support behavior change for improved health status.16
To apply BMI during patient discussions, as in those related to HPV, dental hygiene students need training in basic MI skills and the delivery of BMI. Motivational interviewing training including coaching, role-playing, and feedback have been found to increase retention of skills and provider confidence.19,20,22 Croffoot et al. reported dental hygiene students’ use of open-ended questions, affirmation, reflection and summaries improved with coaching and feedback,17 while Stull et al. found that students need continuous training to feel confident having HPV discussions during patient care.11
Oral health care professionals have expressed an interest in communication training for HPV-related discussions during patient care.6,10,13,14 There is a gap in the literature regarding the most effective communication strategy for discussions regarding a sexually transmitted infection. It is also not known how to best prepare future oral health care providers, such as dental hygiene and dental therapy students, for discussions regarding HPV. The purpose of this study was to examine dental hygiene and dental therapy students’ perceptions of the importance of and their confidence with applying BMI strategies during patient counseling sessions regarding HPV.
Methods
This study was approved by the Institutional Review Boards of A. T. Still University (IRB #2019-106) and the University of Minnesota (STUDY00007617). A convenience sample of dental hygiene and dual degree dental hygiene/dental therapy students (n=32) from the University of Minnesota (UMN) participated in an enhanced HPV BMI curriculum over two semesters. Motivational interviewing is a thread within the UMN curriculum program that encompasses both dental hygiene and dental therapy students beginning during the second semester and has been detailed previously.11
The BMI HPV communication training included a multimodal 40-minute online educational module on general HPV information, the role of HPV in OPC, and HPV vaccination fact sheet. Following the HPV online educational module, students participated in a 90-minute HPV BMI coaching and role-playing session facilitated by an HPV faculty expert (CS) and an MI trained DH educator (MA). During the 90-minute session, students were coached on the utilization of eight MI strategies: 1) open-ended questions, 2) affirmation, 3) reflection, 4) summarize, 5) change talk, 6) use of the importance ruler, 7) ask for elaboration, and 8) enhance self-efficacy to apply during HPV discussions with patients. In addition, students were trained on the MI technique of elicit-provide-elicit (E-P-E). Students were paired into partners for role-plays as the patient and oral health care provider while practicing the eight MI strategies and E-P-E.
Students had four assignments spanning two semesters that included audio-recorded HPV BMI discussions (interactions) during clinical care with two patients followed by two self-assessment assignments. The two self-assessments were completed after listening to the audio recordings and grading their application of BMI for the HPV discussions using the UMN standardized HPV MI rubric. The audio recordings were also team graded by CS and MA using the same rubric. The standardized rubric focused on the four components of the spirit of MI and also included asking permission, and RULEs. The team grading served as an outcome measure of MI fidelity to ensure that the MI strategies were used during the HPV discussions.
Students’ perceptions of the importance of and confidence with applying BMI during HPV patient counseling were measured by three evaluation instruments: pre-test, post-test 1, and post-test 2. The previously validated evaluation instruments were adapted with permission from the University of Missouri Kansas City and the University of Michigan and have been used for numerous studies measuring dental hygiene students’ perceptions of importance and confidence in using MI strategies.17–20 The three questionnaires were revised to have a focus on HPV related topics and were piloted tested by six faculty at the UMN School of Dentistry. Revisions were included to enhance the clarity of the evaluation instruments. All three evaluation instruments included Likert six-point scale questions; the post-tests also included open response items.
The pre-test was delivered prior to the 90-minute HPV BMI coaching and role-playing session. The pre-test addressed students’ perception of the importance of and confidence with applying the eight MI strategies, students’ perspective of using MI for HPV, OPC, and vaccine uptake discussions, and their confidence in applying the spirit of MI. The first post-test was delivered immediately following the 90-minute coaching and role-playing session and included the same questions from the pre-test along with additional items to determine the student’s perspective of the enhanced HPV BMI curriculum. Students then completed two audio-recorded patient interactions on HPV, followed by two self-assessments using the HPV MI rubric. After receiving faculty feedback via the team-graded HPV MI rubric, students then completed the second post-test. The post-test 2 included all the items from post-test 1 with additional items to evaluate the students’ perspectives of their HPV patient interactions, self-assessment, and faculty team-graded feedback.
Responses were compared between the three testing time points using linear models. Pairwise comparisons between time points were adjusted for multiple comparisons using the Tukey method. The patient interaction team graded HPV MI rubrics were compared between interactions one and two using mixed effects linear models with a random effect for each student. Responses and grades were summarized using means, standard deviations, and confidence intervals. Data analysis was performed using an online statistical software program (R version 4.0.1). A two-sided p-value less than 0.05 was regarded as statistically significant.
Results
A total of 32 students (dental hygiene n=24, dental hygiene/dental therapy n=8) completed three evaluation instruments at different time points during their HPV BMI training (n=34). Participants’ perception of the importance of BMI increased at post-test 1 and post-test 2, as compared to the pre-test, for the strategies: Listening Reflectively (pre-test, 5.69±0.69; post-test 1, 5.77±0.63; post-test 2, 5.72±0.55), Elicit Change Talk (pretest, 5.53±0.67; post-test 1, 5.60±0.77; post-test 2, 5.62±0.66), and for the Use of the Importance Ruler (pre-test, 5.35±0.80; post-test 1, 5.43±0.73; post-test 2, 5.38±0.75). However, no statistical significance was found for students’ perceptions of the importance of the eight MI strategies over three time points (Table I).
Perceptions of the importance of and confidence with applying the eight MI strategies during HPV patient counseling* (n=32)
Participants’ perceptions of confidence with applying BMI strategies during HPV patient counseling increased over all three time points for the following strategies: Use of Open-Ended Questions (pre-test, 4.75±1.16; post-test 1, 5.00±1.03; and post-test 2, 5.00±0.98), Make Affirmations (pre-test, 4.94±0.98; post-test 1, 5.06±0.93; and post-test 2, 5.28±0.63), and Use of the Importance Ruler (pre-test, 3.97±0.96; post-test 1, 4.77±0.88; and post-test 2, 4.78±0.97). Perceptions of confidence with applying BMI strategies increased from pre-test to post-test 1, but decreased by post-test 2 for the strategies: Listen Reflectively (pre-test, 5.34±0.79; post-test 1, 5.42±0.72; post-test 2, 5.00±0.98), Elicit Change Talk (pre-test, 4.06±0.95; post-test 1, 4.52±1.09; and pre-test 2, 4.50±1.14), Ask for Elaboration (pre-test, 5.03±0.93; post-test 1, 5.16±0.97; post-test 2, 4.90±1.01), and Enhance Self-Efficacy (pre-test, 4.56±0.88; post-test 1, 5.03±0.84; post-test 2, 4.88±0.91). Statistical significance was found for the Use of the Importance Ruler (0.003) from pre-test to post-test 1 and pre-test to post-test 2 (0.003). Participants’ perception- of the importance of and confidence with applying the eight MI strategies over three time points is shown in Table I.
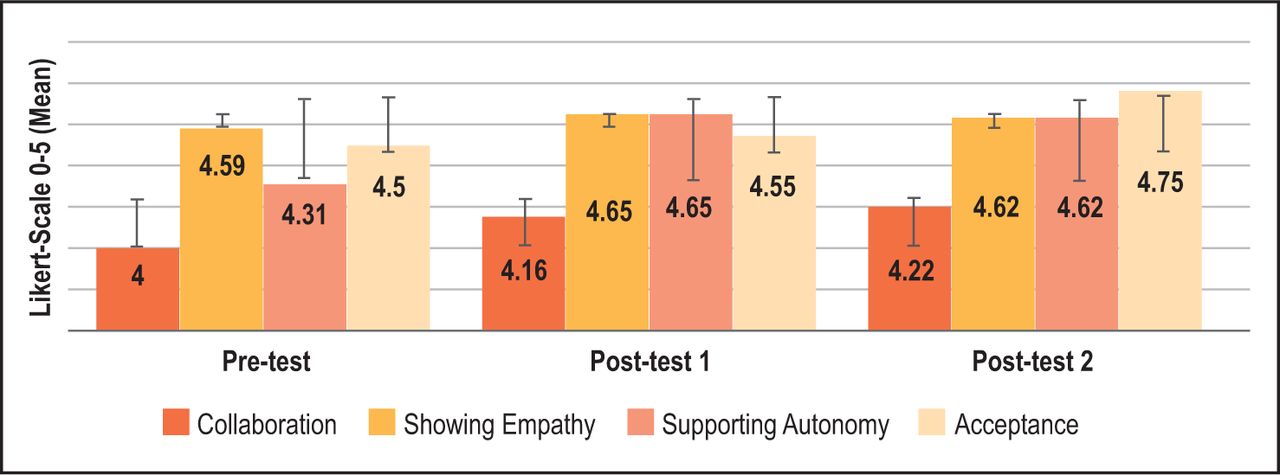
Participants’ perceptions of confidence with demonstrating collaboration (pre-test, 4.00±0.95; post-test 1, 4.16±0.82; and post-test 2, 4.22±0.61) increased over all three time points but was not statistically significant. Perceptions of confidence with demonstrating acceptance (pre-test, 4.59±0.72; post-test 1, 4.65±0.68; and post-test 2, 4.62±0.51), showing empathy (pre-test, 4.59±0.80; post-test 1, 4.65±0.61; and post-test 2, 4.62±0.61) and “-supporting autonomy (pre-test, 4.31±0.86; post-test 1, 4.65±0.66; and post-test 2, 4.62±0.55) increased from pre-test to post-test 1, but decreased from post-test 1 to post-test 2 and was not statistically significant. Participants’ confidence with demonstrating the “Spirt of MI” is illustrated in Figure I.
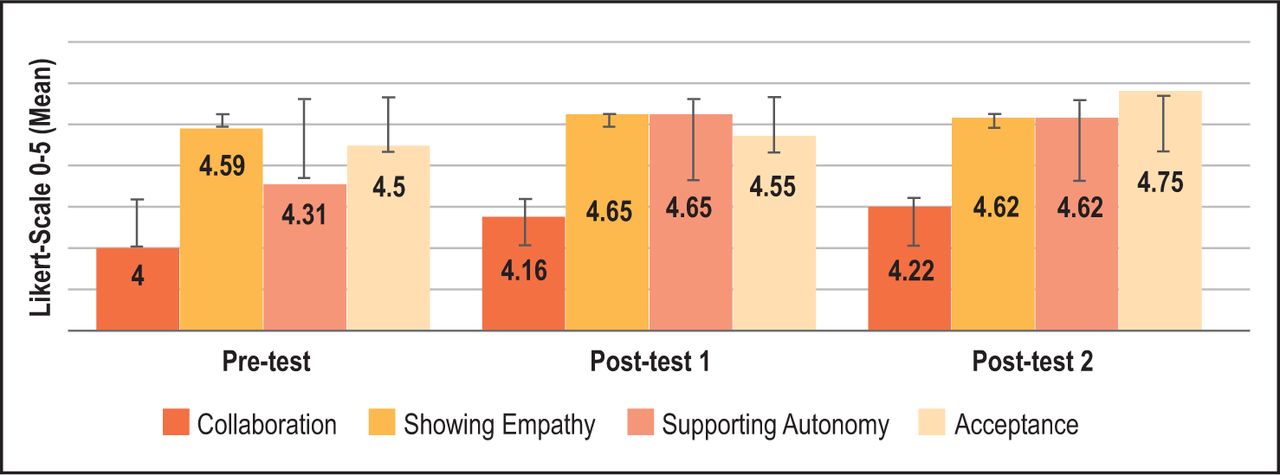
Confidence demonstrating the spirit of MI* (n=32)
Perceptions that “BMI will be a valuable strategy that can be used during clinical care to educate patients about HPV” slightly decreased over three time points (pre-test, 5.69±0.59; post-test 1, 5.58±0.76; and post-test 2, 5.31±0.82). Respondents reporting that “using MI will help my patients understand the HPV-oropharyngeal cancer relationship, risk factors, and prevention, including vaccination” increased from pre-test (5.56±0.76) to post-test 1 (5.58±0.62) and decreased from post-test 1 to post-test 2 (5.25±0.80). Respondents’ perceptions increased from pre-test (4.09±1.17) to post-test 1 (4.83±1.02) and decreased by post-test 2 (4.62±1.01) for the statement, “I have enough time in clinic to incorporate MI strategies for HPV patient education and vaccine advocacy” and statistical significance was found from pre-test to post-test 1 (p=0.02). Perceptions increased for the statement, “I have the skills I need to use MI strategies in the clinic for HPV patient education and vaccine advocacy” (pre-test 4.50±0.92; post-test 1, 4.74±0.82; and post-test 2, 4.88±0.83) but were not statistically significant. Students’ perceptions of BMI during HPV patient discussions are provided in Table II.
Perceptions of MI during HPV patient counseling* (n=32)
Participants’ perceptions of the HPV and the BMI content were evaluated from post-test 1 and post-test 2. Perceptions of the HPV and BMI content decreased from post-test 1 to post-test 2. Statistical significance was found for the statement, “The material covered in DH 3123 was sufficient in detail for me to understand the application of MI to HPV discussions” (p=0.02) and “The HPV and MI activities were an effective way for me to demonstrate my MI skills” (p=0.01). Post-test 2 provided an opportunity for students to report challenges they experienced during HPV patient interactions (Table IV). Frequently reported themes of challenge included difficulty with MI strategies, patient resistance, and uncomfortable being recorded.
Perceptions of HPV and MI content* (n=32)
Challenges during HPV patient counseling (n=32)
Faculty evaluation and students’ self-assessment scores from the standardized HPV MI rubric are shown in Table V. The faculty evaluation mean score for the first patient interaction was 20.9/30 (95% confidence interval (CI) 18.9-22.9) and the second interaction was 24.8/30 (95% CI 22.7-26.8); the difference between the two interactions was 3.8 (95% CI 1.3-6.4, p=0.004), demonstrating a statistically significant improvement in BMI skills over time. The self-assessment score for the first patient Interaction was 20.1/30 (95% CI 18.6-21.7) and the second Interaction was 22.9/30 (95% CI 21.1-24.7); and the difference between the two interactions was 2.9 (95% CI 0.8-5.5, p=0.008), demonstrating a statistically significant improvement.
HPV MI rubric scores* (n=32)
Discussion
This study examined students’ perceptions of the importance of and confidence with applying eight MI strategies and practicing the “Spirit of MI” during HPV related BMI discussions. While not statistically significant at all three time points, most of the participants in this study reported their perception of the importance of applying the eight strategies as “high” during HPV BMI patient counseling, aligning with previous research findings of Croffoott et al.17 Research by Mills et al. also reported findings of students’ perceptions of the importance of the MI strategies of open questions, making affirmations, summarizing, and enhance self-efficacy during preventive education.20 However, unique to the current study, was the incorporation of discussing a sexually transmitted infection as part of the BMI interaction with a patient, which may have impacted exact comparisons to previous MI and BMI studies. Stull et al. reported students’ lack of HPV knowledge and inexperience using BMI techniques impacted confidence when discussing HPV related topics during patient care.11 However, in a study of health care providers use of MI techniques in adolescent HPV vaccination conversations with parents, open-ended questions, reflections and affirmations were used most frequently and were associated with increased perceptions of vaccination acceptance rates.10
Perception of confidence with applying the eight MI strategies during patient care was slightly lower as compared to the ratings of importance of the strategies at all three time points, similar to the findings of Mills et al.20 While students may be supportive of the strategies and view them as important communication tools, due to inexperience they may be less confident in applying them in practice. Participants in this study rated the MI strategies “high,” which over time, may lead to improved confidence during HPV discussions with patients. This lack of confidence is not limited to students. Arnett et al. reported dental hygiene faculty had lower levels of confidence in applying the MI strategies as compared to the importance of supporting students’ delivery of the strategies Elicit Change Talk, Ask for Elaboration, and Enhance Self-Efficacy.19 Using a variety of faculty development activities with appropriate follow-up is needed for ensuring long-term effects and maintaining confidence.
In this study, confidence with the “Use of Importance Ruler” was the only MI strategy to achieve statistical significance, whereas Mills et al. reported significance of students’ confidence with seven of the eight MI strategies over time.20 Previous studies have investigated the use of MI knowledge during HPV discussions, but have not explored levels of provider confidence with the application of the strategies.10,13,14 As this is a novel study assessing perceptions of confidence with applying BMI during HPV discussion, it is difficult to identify why the Use of Importance Ruler was statistically significant as compared to the other MI strategies. Participants may have been confident with this strategy because it was taught during the role-playing session as a way to assess patients’ interest and readiness to discuss the HPV vaccine with their primary care physician. The Use of the Importance Ruler is a scale similar to the Visual Analog Pain Scale, a familiar tool in their professional student role and an easy way to assess HPV vaccine interest. It has been well documented in the literature that oral health care providers report limited confidence and communication skills for discussing HPV-related topics with patients4,6,8–11 and this may be even more of an issue with oral health care students. Furthermore, the gap in time from the HPV BMI coaching and role-playing session to clinical application during the two patient interactions may have been too long to maintain perceptions of confidence with applying MI strategies to HPV discussions. These findings align with the literature that to be effective using MI, it requires training, coaching, and feedback to retain confidence and long-term skills.19,20,22
Open responses from students indicate patient resistance as a challenge. This may be related to students in this study not applying the MI RULES, to mitigate patient resistance. Students lost points on the UMN standardized HPV MI rubric in the categories of collaboration and evocation for lecturing the patient and not supporting patient autonomy. Patient selection may have also impacted students’ perceptions of challenges reported in this study. The patient criteria for the audio recordings were men and women between the ages of 18 and 45. The UMN SOD has a large geriatric population, making it difficult for students to complete the two HPV assignments with patients meeting the age criteria. Therefore, students may have sought patients meeting the age criteria only without considering patient-provider trust and rapport, the foundation of the “Spirit of MI.” Building patient-provider trust and rapport takes time and is not achieved with one interaction. As a potential explanation, students with unestablished trust and rapport may have enhanced patient resistance, especially because HPV, HPV vaccine uptake, and HPV as it relates to OPCs are sensitive topics to discuss with patients. Patients may not have understood the connection between HPV and oral health or the reason their student providers initiated the discussion, leading to resistance. Further, students’ perceptions of “confidence” with showing empathy was less over time compared to collaboration, acceptance, and supporting autonomy. The decrease in “confidence” with demonstrating the ability in showing empathy may be a result of patient resistance.
While perceptions of the importance of and confidence with applying the majority of the eight MI strategies, was not statistically significant in this study, the self-assessment scores from the first to second patient interaction increased with statistical significance. Similarly, faculty evaluation of students’ patient interactions also improved overtime with statistical significance. The patient interactions and self-assessments were low stake assignments for students and earning a high score on the standardized HPV MI rubric had little to no impact on their overall course grade. Despite limited performance incentives, similar scores were reached between the faculty evaluations and the students’ self-assessment. Perceptions of the importance of and confidence in applying the MI strategies coupled with the students’ self-assessment scores supports prior research demonstrating the efficacy of MI strategies and the spirit of MI for discussions related to HPV vaccination strategies.
This study had limitations. The sample was from one institution at a Midwestern dental school with no control or comparison group and the results cannot be generalized. The validated pre-test and post-tests 1 and 2 were revised to include HPV specific content. While the revised instruments were pilot tested, they were not revalidated. Confounding factors such as confidence with and comfort discussing HPV topics with patients may have influenced students’ perceptions regarding the importance of and confidence with applying MI strategies and the use of unpaired data to maintain anonymity may have impacted the ability to achieve statistical significance.
Conclusion
Findings from this study indicate a 90-minute BMI coaching and role-playing session and self-assessments along with faculty feedback from two patient interactions, is not enough training to retain long-term confidence with applying MI strategies during HPV discussions. Refresher training in BMI for HPV conversations as part of patient care should be implemented prior to clinical application. Perceptions of confidence and comfort discussing HPV topics may have impacted student confidence in applying MI strategies. Additional MI experiences using objective structured clinical examinations (OSCE) with standardized patients to practice BMI HPV discussions and faculty evaluation should be explored.
Acknowledgment
The authors would like to thank the University of Missouri-Kansas City and the University of Michigan Dental Hygiene Programs for their contributions to MI research. We also want to thank Kimberly Krust-Bray and Angela Mills for permission to modify their evaluation instruments to allow us to carry out this important work.
Footnotes
This manuscript supports the NDHRA priority area Professional development: education (educational models).
Disclosure
This study was supported by the National Institutes of Health’s National Center for Advancing Translational Sciences, grant UL1TR002494. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health’s National Center for Advancing Translational Sciences.
- Received April 12, 2021.
- Accepted June 8, 2021.
- Copyright © 2022 The American Dental Hygienists’ Association





{kind=link}