



Abstract
Purpose: The COVID-19 pandemic has led to drops in patient volume and staffing in dental practices in the United States (US). This study aimed to provide insights on dental hygienists’ employment patterns as well as their attitudes toward working as dental hygienists during a pandemic.
Methods: Licensed dental hygienists were invited to participate in a web-based 30-question survey between September 29 and October 8, 2020. Employment questions included current and pre-pandemic work status, reasons for not currently working as a dental hygienist, and estimated levels of personal protective equipment (PPE) in the primary work location. All statistical analysis was conducted in Qualtrics Core XM; cross tabulation was used to examine dental hygienist working patterns and attitudes by age, practice PPE supply, and other factors.
Results: The COVID-19 pandemic has led to an estimated 8% reduction in dental hygienist employment. The majority (59.1%, n=205) of this reduction is voluntary, with the main reason being general concerns over COVID-19 (48.3%, n=100). Other reasons include issues surrounding childcare and concerns over safety measures in the workplace. Dental hygienists aged 65 and older were most likely to have left the workforce voluntarily. More than half of respondents reported that their work locations had more than a two-week supply of most PPE items, although about 10% did not know supply levels. Dental hygienists working in settings with lower supplies of PPE were more concerned with COVID-19 transmission risk to themselves or to patients.
Conclusion: COVID-19 has led to a reduction in the dental hygienist workforce that is likely to persist until the pandemic passes.The dental hygienist labor market has tightened and employers may continue to experience difficulties in filling vacant dental hygienist positions until the pandemic subsides. There is also likely to be a longer term, yet smaller, impact on dental hygiene employment levels.
Introduction
The COVID-19 pandemic is having a major effect on the dental care delivery system in the United States (US). Patient volume in dental offices fell to about 7% of typical levels during the period when dental offices were closed. Subsequently, it has rebounded, but not completely. The latest data, in fact, suggest that dental patient volume will remain at about 80% of pre-COVID-19 levels, at least until a vaccine or proven treatment is available.1 Employment in dental care settings, including private practices, dropped by more than half during the period of the dental care shutdown from March to May 2020 and has since stabilized at about 98% of pre-COVID-19 levels, as of October 2020.2 The decline and subsequent rebound in patient volume in the dental care sector stemming from the pandemic is unprecedented in the history of dentistry as well as compared to other sectors of health care. Occupations in dentistry were identified early in the pandemic as occupations with higher-than-average risk for infection.3 In fact, dental hygiene itself was identified as one of the most at-risk non-hospital occupations during a pandemic, with a rating of 99.7 of 100 due to contact with others, physical proximity with others, and exposure to disease and infection.3
The pandemic has had a significant effect on the United States (US) labor market, particularly among women. A variety of factors, including school and daycare closures, the unequal burden of caring for aging parents, and risk of infection being higher in female-dominated occupations, have caused a major exit of women from the labor force in general. These effects could be long lasting, persisting even after the pandemic comes under control.4 Dental hygiene has been well documented as a female-dominated profession, with men making up only 4% of the workforce.5
Little is known about the employment patterns of dental hygienists since the pandemic began. A recent study conducted by the International Federation of Dental Hygienists (IFDH) from May 5 to May 31, 2020, examined over 9,800 dental hygienists from 30 member countries. At that time, results indicated that 52% of the respondents were not working at all due to COVID-19, while 41% were providing some form of in-office clinical care. Further, 50% either agreed or strongly agreed that they were concerned about being unemployed. In the IFDH study, 20% were neutral on employment issues and 30% either disagreed or strongly disagreed regarding concerns related to unemployment.6 No other information about employment patterns were addressed.6 Dental hygienists in Italy completed an online survey during May 2020 to ascertain personal data, protective measures, awareness and risk perception related to COVID-19. The only reference to employment patterns noted in the study was that 63.13% of the respondents stopped working for at least three weeks when the pandemic began in February 2020.7
In comparison, since the onset of the COVID-19 pandemic, there have been regular analyses of its impact on dentists. In late March, the American Dental Association (ADA) Health Policy Institute (HPI) began tracking thousands of dentists and regularly reported on their employment and practice status, their patient volume, and their staffing levels.8 These ongoing analyses have been invaluable in providing a data-driven, empirical snapshot of how the pandemic is affecting dentists in the US. Beginning in September 2020, the American Dental Hygienists’ Association (ADHA) partnered with HPI to begin tracking similar data for dental hygienists. One study, a companion paper to this work, reported estimates of the prevalence of COVID-19 among US dental hygienists, infection prevention and control procedures, and associated trends in mental health. In this paper, the impact of the COVID-19 pandemic on the labor market for dental hygienists is examined. The purpose of this study was to investigate how the COVID 19 pandemic has affected employment patterns of US dental hygienists and their attitudes toward the perceived risks associated with working as a dental hygienist.
Methods
An anonymous web-based survey was administered using Qualtrics (Qualtrics, Provo, UT) from September 29 to October 8, 2020. Licensed dental hygienists based in the US were invited to participate in the study if they were age 18 years or older and employed as a dental hygienist as of March 1, 2020. A total of 133,000 dental hygienists, who were subscribed to the ADHA email listserv, were invited to participate in the survey. Of this group, 4,804 dental hygienists volunteered to participate. The survey was sent on September 29, 2020, and a reminder email was sent on October 6, 2020. The research protocol and survey were approved by the ADA Institutional Review Board and registered at clinicaltrials.gov (NCT04542915).
Potential participants read and signed an electronic informed consent document before responding to the study. A 30-question survey was constructed for this study and was similar to the survey of US dentists.9 In the original survey, the test-retest reliability was on average 85.4%, based on the first two months of identical questions among a panel of dentists.9 Demographic survey questions included age, race/ethnicity, gender, primary practice location, and years of experience as a licensed dental hygienist. Employment questions included current and pre-pandemic work status, reasons for not currently working as a dental hygienist, and estimated levels of personal protective equipment (PPE) in the primary work location. Level of concern about COVID-19 transmission to patients and to themselves in the workplace was assessed using a 5-point scale (1 = very concerned; 5 = not concerned at all). Items related to COVID-19 infection were also included in the survey and were analyzed in a separate paper.
All statistical analysis was conducted in Qualtrics Core XM. Descriptive characteristics were used to describe dental hygienists’ employment status, PPE levels, and concerns regarding COVID-19 transmission to patients and self. Cross tabulation analysis included reasons for not working by age group, level of concern for patients and self by the supply of N95/KN95 masks in primary work location, pre-pandemic and current employment status by age group, and employment status by primary work location type. Differences between non-normal continuous variables were tested using Kruskal-Wallis tests and between categorical variables with X2 tests, with statistical significance set at 0.05 and were conducted in Stata 13.0 (StataCorp LP, TX, USA). Text analysis was performed on two open-ended responses for dental hygienists with other reasons for not currently working in the profession.
Due to complex survey question skip patterns and because respondents were able to skip any non-screening question or stop answering the survey at any time, not all respondents answered all questions. The missing response rate ranged from <1% to 9% per question.
Results
Of the 4,804 dental hygienists who originally volunteered to participate in the survey, 4,776 respondents from all 50 states and Puerto Rico agreed to the informed consent and completed the survey for a completion rate of 99.4%. Respondents were female (98.1%, n=4,034), 18 to 77 years of age (mean: 44.1, standard deviation: 12.0) and predominantly non-Hispanic White (72.5%, n=4,066). Almost one-third of the sample (31.9%, n=1,523) had at least one medical condition associated with a higher risk of developing severe illness from SARS-CoV-2.10 The majority of respondents were employed in a private solo practice (52.5%, n=2,161) or other dental practice (38.4%, n=1,581) while a small percentage of respondents were employed in public health settings (4.5%, n=185), academia (2.8%, n=115) or other areas (1.8%, n=73); 70.3% (n=3,357) of the responding dental hygienists had provided dental care to patients in the month before the survey. Table I highlights the demographic information.
Sample demographics (n=4776)
Dental hygienists participating in the survey were asked their employment status on March 1, 2020 (before the closure of dental practices in the US due to the COVID-19 pandemic) and their current employment status at the time of the survey, which corresponded to the first week of October. A decrease was found in the percentage of dental hygienists employed full-time from March 1 (65.7%; n=3,072) and at the time of the survey (59.0%; n=2,679). Among the respondents employed part-time, this percentage remained constant, standing at 30.4% (n=1,423) on March 1 and 31.1% (n=1,414) at the time of the survey (Table II).
Employment status among respondents pre-COVID-19 (n=4674) and currently (n=4543)
Changes in employment status pre- and post-COVID differed by age group, with older dental hygienists affected more significantly. Among dental hygienists age 65 and older, the percentage employed full-time decreased by 11.2 percentage points compared to 6.2 percentage points among dental hygienists under age 35 (X2 p value: 0.001). Nearly one-quarter of respondents over age 65 (n=41) reported they are not currently employed as a dental hygienist compared to 5.8% of the respondents under age 35 (n=60) (Table II).
Among the respondents currently employed in the workforce, three in five (n=2,484) reported they are working the same number of hours as they were before the pandemic began, whereas one-fifth (n=899) reported working reduced hours. For those respondents working in solo dental practices, nearly one-quarter (n=489) reported working reduced hours, compared to 11.9% (n=19) of respondents working in dental service organizations (DSOs), 19.0% (n=216) in group dental practices, and 16.4% (n=29) in public health clinics or federally qualified health centers. In fact, one-fifth of the respondents employed in DSOs (n=32) reported working more hours than before the COVID-19 pandemic.
Nearly one in twelve respondents (7.9%; n=360) who were employed as dental hygienists on March 1 reported they have since left the workforce. Within this group, 59.1% (n=205) reported leaving their dental hygienist position voluntarily while 24.1% (n=84) were laid off/furloughed and 16.7% (n=58) were permanently let go. There were also important differences by age, though not statistically significant (X2 p-value: 0.3). Respondents over age 65 were more likely to report having voluntarily left their positions (68.3%; n=28) compared to respondents under age 35 (53.3%; n=32). Over one-quarter of respondents age 45-54 reported that they were permanently let go from their positions.
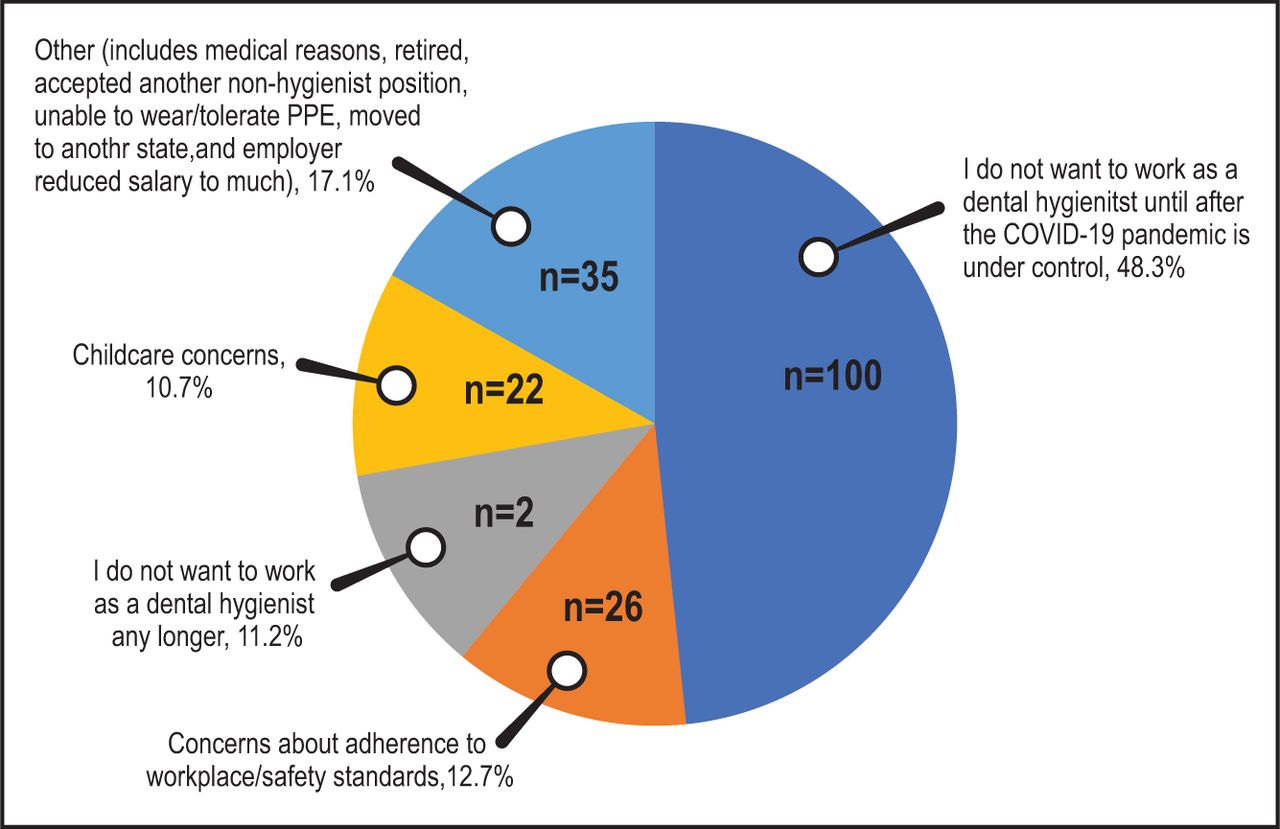
Among the respondents who voluntarily left their positions, the most common reason given was not wanting to return to work until the COVID-19 pandemic is under control (48.3%; n=100). Other reasons included concerns about adherence to workplace/safety standards at their place of employment (12.7%; n=26), no longer wanting to work as a dental hygienist (11.2%; n=23), and childcare concerns (10.7%; n=22) (Figure 1).

Reasons cited for voluntarily leaving a dental hygiene position (n=205)
Among respondents who were let go from their positions, 35.9% (n=51) reported that they have not returned to work because they preferred to wait until the COVID-19 pandemic is under control. Equal numbers of respondents (11.3%; n=16) reported they have not yet found another position or are waiting to be rehired by their original practice setting.
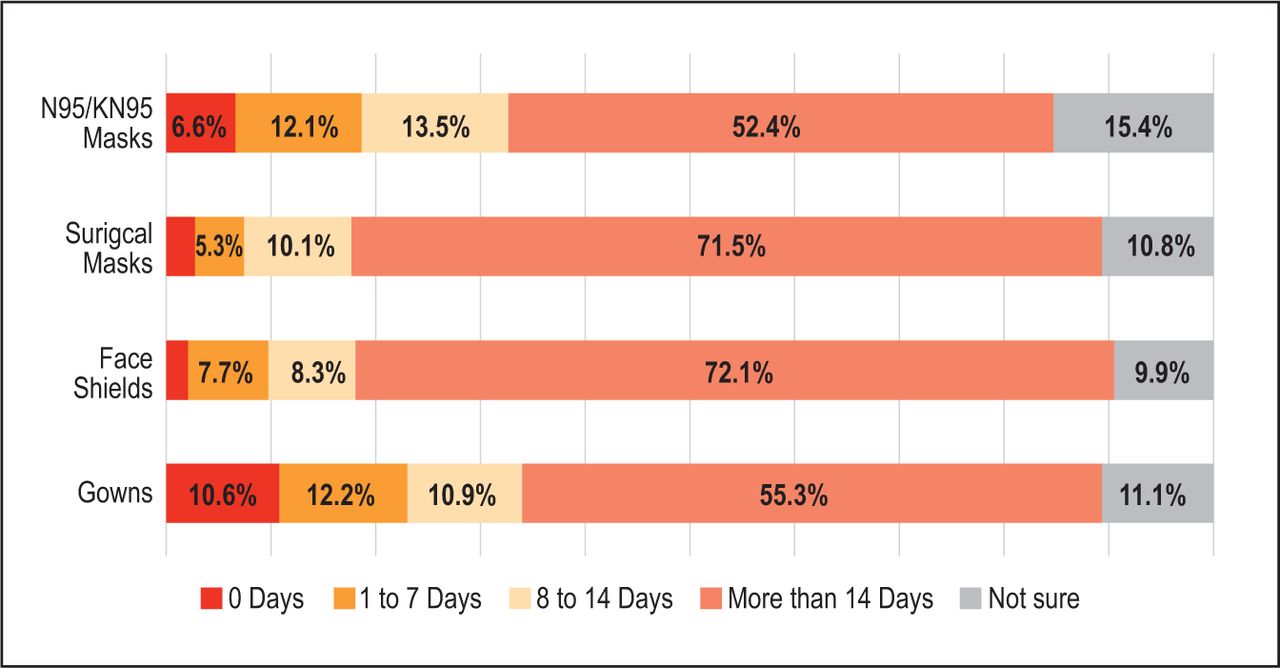
Some respondents who have become unemployed since March 1 (whether voluntarily or not), cited concerns over the ongoing pandemic and anxiety about workplace safety as reasons for not currently practicing dental hygiene. Respondents who are currently still employed were also asked questions regarding their safety concerns. On a scale of 1 to 5 (1=Very concerned; 5=Not concerned at all), respondents rated their overall concerns regarding the risk of transmission to patients as 3.26 and to themselves as 3.15 (Figure 2). Concerns varied relative to the PPE supply in their primary practice location. Respondents whose practices had two weeks’ worth of N95/KN95 masks or less, were more concerned than respondents whose practices had more than two weeks’ worth of N95/KN95 masks (Kruskal-Wallis p-values <0.001). When examined by age, the level of concern to both patients (3.09) and themselves (2.97) was greatest among respondents age 65 and older; however, the difference was not statistically significant (Kruskal-Wallis p-values>0.1). For all other age groups, there was little variation. It should be noted that for each category of PPE supplies respondents were asked about, about one in ten reported not knowing how many days of supplies their primary work location had. At least half of the respondents (52.4%, n=2,082) reported that their primary work location had more than 14 days of supplies for each PPE category. Nearly seven percent (n=264) of respondents reported that their primary work location did not have any N95/KN95 masks (Figure 3).
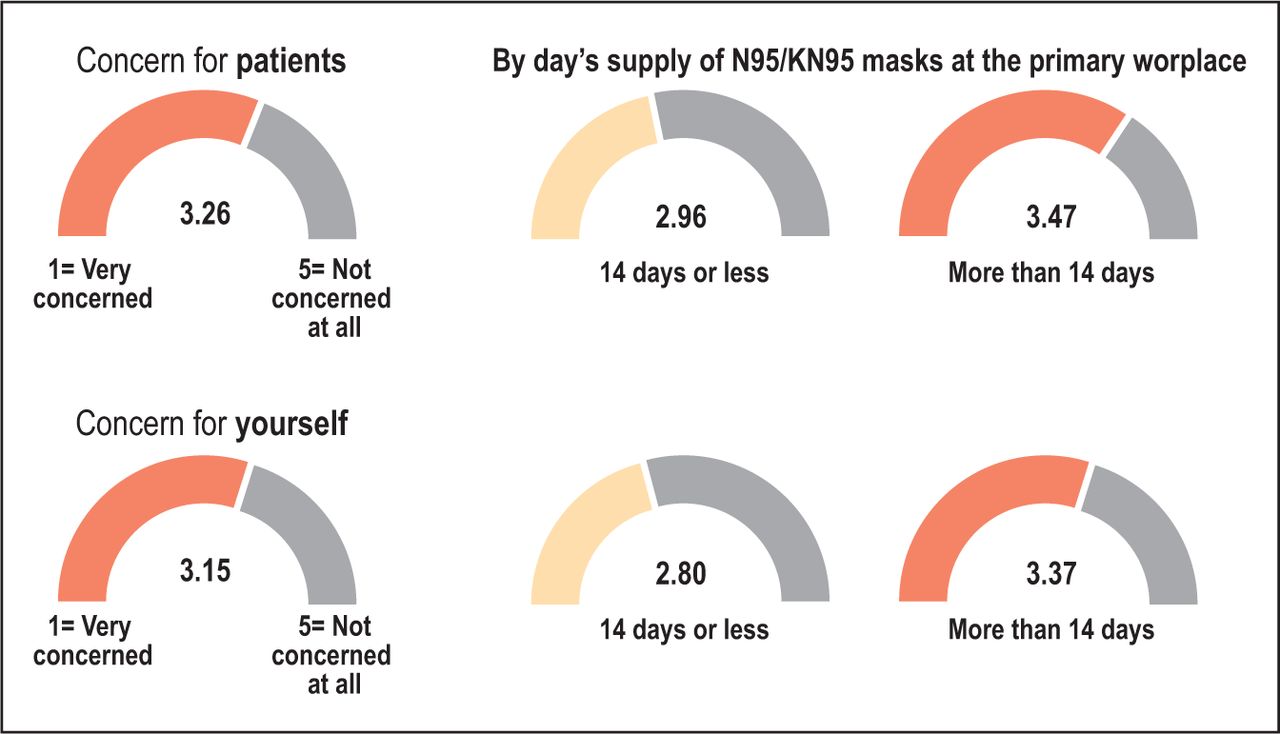
Level of concern regarding risk of COVID-19 transmission in primary work location
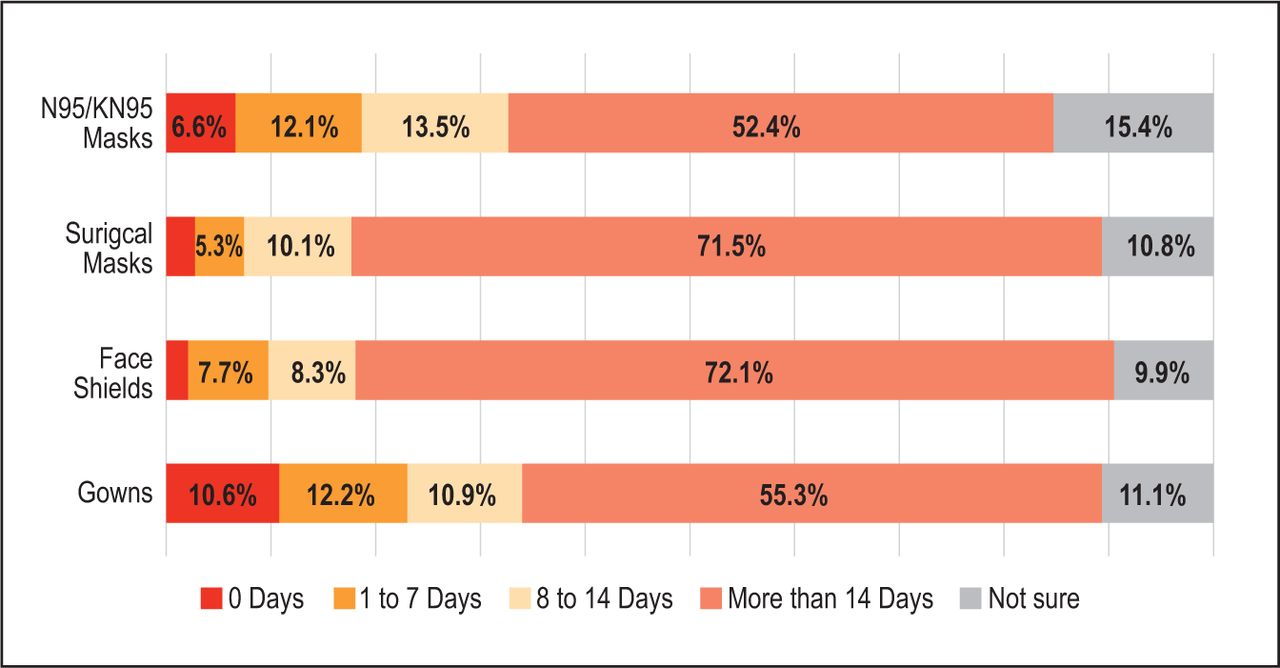
PPE supplies at primary work locationtion
Of 329 respondents who have become unemployed since March 1, more than half reported either receiving unemployment benefits (n=143) or that they have applied for benefits but have not yet received any (n=20). Another 38.3% (n=126) had not applied for unemployment benefits. Over one in ten (12.2%; n=40) reported that their unemployment benefits applications had been denied.
Discussion:
COVID-19 is bringing unprecedented disruption to the US health care sector, including the health workforce. This is the first research to date that explores these issues based on robust, nationally representative data. Analysis of this study indicates that 7.9% of dental hygienists have exited the workforce since the onset of the COVID-19 pandemic. This translates to an estimated reduction of 18,000 dental hygienists from the workforce. Dentists have indicated that the dental hygiene labor market has tightened considerably; data collected for the week of October 5 indicate that one-quarter of dental offices reported they had recently hired or were actively recruiting dental hygienists.8 Among these dentists, more than three-quarters reported it was extremely or very challenging to fill vacant dental hygienist positions.8 An estimated 90% of dentists received some type of financial relief from the federal government, including the Paycheck Protection Program, and this contributed significantly to maintaining demand for dental hygienists.
A key insight from this research is that the majority of dental hygienists in this study who left their jobs did so voluntarily. Further analysis suggests that most of this voluntary departure from the workforce is likely to be short-term or, more formally, lasting through the COVID-19 pandemic. But there is also a portion of dental hygienists who indicate they do not want to be employed as a dental hygienist any longer, even after the COVID-19 pandemic is under control. Results indicate that at least 0.5% of the dental hygiene workforce may be in this category of permanently leaving their jobs. Further investigation is needed to understand factors associated with dental hygienists’ decisions to leave clinical practice. A qualitative study may illuminate dental hygienists’ perceptions and plans to pursue other careers within the profession, find alternative career options outside of dental hygiene, or remain unemployed.
Another relevant finding is the issue of age and association with employment status. Results revealed that more dental hygienists age 65 years and older were not currently employed or voluntarily left their positions. Further study is needed to understand if there is a relationship between these individuals and those with comorbidities that place them at greater risk for SARS-CoV-2.10 Respondents’ choice to remain out of work could have been impacted by physical health concerns and associated COVID-19 illness. Further study is also needed among dental hygienists age 45-54 who indicated they were permanently let go and the rationale for their termination.
The results of this study also provide additional evidence of how COVID-19 is bringing unique challenges to women in the workforce. Dental hygiene has traditionally been a female-dominated profession and these results provide another example of how childcare issues are playing an exaggerated role during the COVID-19 pandemic in driving career choices. While these unique childcare issues are likely to resolve as the pandemic subsides and schools and childcare facilities reopen, there is emerging evidence that COVID-19 may have long-term consequences for earnings and career prospects of women.11
Regarding dental hygienists’ concern for contracting COVID-19 in the workplace, this study confirms PPE availability is an important factor. Dental hygienists with higher stockpiles of N95 or KN95 masks in their place of employment reported lower levels of concern. Further, analysis also found that a small percentage of dental hygienists did not actually know how many days’ worth of N95 of KN95 masks were in stock at their place of work. This finding is concerning because participants may be making decisions regarding their employment status without full knowledge of PPE availability and not utilizing national guidance to evaluate whether supplies are sufficient for patient volume.
Concern over adherence to workplace safety standards, which could reflect PPE practices as well as many other factors, was also important for 13% of the participating dental hygienists in terms of influencing their decision to voluntarily leave their job. In the recent ADA study, researchers found that 99% of dental offices in the US were using some form of enhanced infection control as a result of COVID-19 and that 73% were using PPE according to interim guidance from the Centers for Disease Control and Prevention (CDC).9 While PPE stockpiles in dental practice settings have improved considerably in the past months, certain items such as N95 masks and gowns are still in relatively short supply.9 Reference to PPE shortages appears to be a worldwide concern. Dental hygienists responding to the survey conducted by the IFDH demonstrated that current PPE was limited in terms of goggles (46%) and full gown (48%), and not all practitioners were provided gloves (86%), face shields (76%), or surgical masks (69%).6 Over 80% of the international respondents expressed concern that there would not be an adequate supply of PPE to treat patients.6
Lastly, with the onset of administration of vaccines in the US, some dental hygienists may decide to reenter the workforce in the near future. Two vaccines, mRNA-1273, (Moderna, Inc.) and BNT162b2 (Pfizer BioNTech) have received emergency use authorization from the US Food and Drug Administration, and are being provided to health care workers and residents in long-term care facilities.12 Dental and dental hygiene national associations have advocated for oral health care workers to be among the first groups to receive the vaccine recognizing that they are essential health care workers and play a critical role in addressing significant oral and systemic health conditions.13-15 Furthermore, dental hygienists can also play a primary role in addressing COVID-19 by being part of the CDC vaccination response. Administering vaccines, as recently approved in the state of Connecticut,16 and educating patients about the need for vaccination for pandemic prevention and control, are examples of measures illustrating ways dental hygienists can support positive changes in addressing the COVID-19 pandemic in workplace settings.
This study is not without limitations. The research is based on self-reported data, which may be influenced by recall or social desirability bias. However, this study represents only the beginning of an ongoing effort to understand the impact of COVID-19 on the employment of dental hygienists. Future research using data from this longitudinal study will continue to examine employment factors among dental hygienists in the US and determine the extent to which the COVID-19 pandemic has a permanent effect on their employment. Factors that may influence dental hygienists’ decisions to return to work should be further explored from both a quantitative and qualitative perspective.
Conclusion
Results from this study provide the first empirical insight into the impact of COVID-19 on dental hygiene employment. Taken together, the analysis suggests COVID-19 has led to a significant reduction in the dental hygiene workforce that is likely to persist until the pandemic passes. The labor market for dental hygienists has tightened, with significant recruitment challenges being reported by dentists looking to hire dental hygienists. Results also indicate there will likely to be a much smaller, but longer lasting impact, as a small share of dental hygienists permanently leave the workforce.
Acknowledgment
The authors wish to thank Brittany Harrison from the ADA Health Policy Institute for her editorial assistance.
Footnotes
This manuscript supports the NDHRA priority area Professional development: Occupational health (Determination and assessment of risks)
- Received December 17, 2020.
- Accepted January 8, 2021.
- Copyright © 2021 The American Dental Hygienists’ Association
This article is open access and may not be copied, distributed, or modified without written permission from the American Dental Hygienists’ Association.





{kind=link}
{kind=link}
{kind=link}