



Abstract
Purpose: Motivational Interviewing (MI) is an evidence-based, patient-centered counseling approach for eliciting behavior change. In 2012, the University of Michigan (U-M) Dental Hygiene Program significantly enhanced their behavior change curriculum by reinforcing and building upon the Motivational Interviewing segment. The purpose of this study was to examine students' perceptions of the importance of MI and their confidence in applying it during patient care.
Methods: A convenience sample of 22 U-M Class of 2015 dental hygiene students who had received an enhanced curriculum participated in this study, utilizing a retrospective, pre-test/post-test design.
Results: A Wilcoxon signed rank test was used to compare the differences in average ranks between T1 (Retrospective Pre-Test) and T4 (Post-Test 3) for the importance and confidence questions at each time point for the Class of 2015. Students' perceptions of importance increased with statistical significance in five out of eight MI strategies. Perceptions in confidence increased in seven out of eight strategies. Effect size ranged from .00 to .55. Assessment of qualitative data provided additional insight on student experiences.
Conclusion: Student perceptions of importance of using MI and their confidence in applying MI increased in a majority of the strategy categories. Successes with patient health behavior change and challenges with time to integrate this in practice were noted. Research on the longitudinal impact and faculty feedback calibration is recommended.
Introduction
Oral health has a significant impact on overall health.1-4 Major oral diseases include dental caries, periodontal diseases, and oral and pharyngeal cancers.1-5 While the majority are preventable, millions of Americans suffer from these debilitating conditions.2-5 Patient adherence to recommended treatments and healthy behavior changes are essential in preventing and treating oral diseases.
The U.S. Department of Health and Human Services developed the Healthy People 2020 initiative to create science-based objectives for improving the health of Americans.3 One of the objectives focuses on promoting quality of life by encouraging healthy behaviors and motivating individuals toward making educated health decisions.3 Significantly, Healthy People 2020 recognizes the need for primary care practitioners to provide health counseling for their patients.3 However, many providers counsel patients using methods of persuasion and confrontation and these methods have been shown to be ineffective.6 According to DiMatteo et al., traditional health behavior recommendations by the clinician are generally not followed and can lead to disappointment for the clinician and a setback for the patient.7
For the purposes of this study, Motivational Interviewing (MI) is defined as an evidence-based, patient-centered counseling approach for eliciting behavior change.8-10 Using a non-authoritative approach focusing on interpersonal communication, MI enables the patient to naturally break through uncertain thoughts, feelings, and attitudes to achieve a positive health behavior change.9,10 Studies incorporating MI into health care curricula demonstrate positive effects on students' abilities to discuss health behavior change with patients.11
In 2012, the University of Michigan (U-M) Dental Hygiene (DH) program embarked on a project to enhance their health behavior curriculum with a special focus on MI. The desired outcome was for students to translate content learned in the classroom to clinical application during patient care. The purpose of this study was to examine U-M dental hygiene students exposed to the enhanced MI curriculum and to assess both their perceptions of the importance of using MI and their confidence in applying it.
Motivational Interviewing
MI is different from traditional methods of behavior change counseling because it focuses on collaboration, not compliance. It empowers the patient and reinforces a positive relationship with the practitioner while offering an individual the autonomy of making their own decisions in an encouraging environment.9,10 In addition, MI application increases the likelihood that patients will adhere to health recommendations.9,10 Positive patient behavior outcomes have been demonstrated to result when health care providers use MI techniques with patients.13-16
The spirit of MI was influenced by the client-centered counseling theory of Carl Rogers, developed in 1953.16 Miller and Rollnick describe this spirit as collaborative, evocative, and autonomous.8 Collaboration between clinician and patient evokes patients' personal motivation, channeling their own values, good reasons, and resources to make lifestyle changes.8 The four main principles of MI are expressing empathy, developing discrepancy, rolling with resistance, and supporting self-efficacy.8,10 In addition, applying MI strategies such as asking open-ended questions, providing affirmation, reflective listening, and summarizing help, elicit change talk, where the patient verbalizes a desire to change.8,10
Application to Oral Health
Most chronic oral diseases are preventable and related to lifestyle choices.2 Oral healthcare practitioners treat acute conditions and also deal with chronic conditions for which the patient is responsible through continued self-management.10 Behaviors contributing to chronic oral diseases such as biofilm removal, poor diet, stress, and tobacco use, can be reshaped with the assistance of an oral health care practitioner.2 These professionals, especially dental hygienists, have repeated interactions allowing the patient and the clinician to build a collaborative relationship.17
A study by Jonsson et al. showed application of MI techniques increased patient compliance with home care and enhanced oral hygiene in those undergoing periodontal therapy.18 Studies by Weinstein et al. revealed children whose mothers received MI counseling related to the child's oral health had fewer carious lesions over time, than children whose parents were not provided with MI counseling.13,14
Brief motivational interviewing has also shown to be effective in health promotion. Brief interventions, between 5-15 minutes long, encourage patient problem solving, elicit change talk, and provide a set of options for planning the next steps of the change.10 Rubak et al. found brief MI to be effective over traditional methods of health behavior change education even when delivered as 15-minute exchanges.19
Incorporating MI into Health Professions Curricula
The complex dynamics of health behavior change is an important concept for practitioners to understand.6,9 With a much greater emphasis on management and prevention of disease, patients are more likely to adhere to treatment when health care practitioners formulate action plans using a patient-centered counseling approach.20 Thus, formal, rigorous training in behavior change counseling is needed for health care practitioners.12 Incorporating MI into health care curriculum has demonstrated positive effects on practitioners' abilities to discuss health behavior change with patients.21
A rigorous curriculum enabling students to have the opportunity to develop these skills is important.9 Knowledge, practice, and experience are also necessary for success.9 Students perform better when they understand the material, have a positive attitude, and have an array of skills gained by practicing.22 Teaching effective interviewing and communication strategies, such as MI, is attained by connecting theory to practice. In order for these strategies to be assimilated, appropriate training and education are needed to give students time to attain skills and develop confidence in applying them.9 Educational activities need to include clinical instruction along with repeated practice, assessment and feedback.22,23
Croffoot et al. studied the effects of coaching dental hygiene students taught to use MI strategies.11 The results indicated that education, in combination with faculty coaching/feedback, provided achievement of core MI skills and increased MI adherence by the students.11 In order to be proficient with MI and develop confidence in its application, exposure is needed early in the curriculum along with continuous reinforcement integrated throughout the entire curriculum.11 Real skill and confidence grow through rigorous practice, feedback, and coaching from a knowledgeable guide.20 MI skills were developed throughout the dental hygiene program as students were developing clinical skills.
Perceptions of Importance and Confidence
Positive student perceptions directly influence learning outcomes and achievement.24 A pilot study by Wiley et al. measured health care practitioners' perceptions of MI training. Practitioners in this study included dieticians, pharmacists, nurses, and social workers.25 Before MI training, their perceptions of health behavior change consisted of low levels of perceived confidence and competence in the ability to help others with feelings of frustration.25 After a 7.5 hour workshop on MI, practitioners' perceptions were assessed and resulted in a renewed inspiration and motivation to facilitate behavior change. Also noted was a desire to partner with patients with less focus on advice giving, a feeling that behavior change is easier and less stressful than anticipated, higher levels of competence and confidence, and greater mindfulness of practitioner impact.25
Students need to value what they are learning, feel it is important, and have the confidence to apply concepts learned. Humair et al. used a self-administered questionnaire to assess students' perceptions of a MI curriculum related to smoking cessation counseling techniques.26 The students participated in two four-hour sessions of smoking cessation training two weeks apart, allowing students time to practice MI and reflect between sessions.26 The results revealed that the students valued the importance of this curriculum and the skills they attained and they also enjoyed their involvement in learning activities.26 White et al. delivered an evaluation to 112 students after the introduction of a MI curriculum consisting of a lecture series and small group discussion, role playing activities, and evaluation of MI video recordings.27 Eighty-three percent of the students felt that the MI curriculum helped them in discussing behavior change with patients and 98% felt it was an important skill for physicians to have.27
Perry et al. assessed the role confidence plays in nursing students' learning.28 This study found that a decrease in confidence unfavorably impacts meeting learning objectives and goals.28 Bell et al. assessed medical students' success with promoting health behavior change through a newly implemented MI curriculum.29 Medical student confidence in utilizing MI was measured after participating in four two-hour training sessions and the student participants were found to be more confident.29 Student confidence has been demonstrated to increase by actually performing skills rather than merely observing them.30
Importance and confidence play important roles in the likelihood that students will incorporate MI into their professional practice.30 The purpose of this study was to examine U-M dental hygiene students exposed to the enhanced MI curriculum and to assess their perceptions of the importance of using MI and their confidence in applying it to patient care.
Materials and Methods
This study was presented to the Institutional Review Board at the University of Michigan. It was approved as “exempt.” A convenience sample of 22 first-year University of Michigan (U-M) dental hygiene students from the Class of 2015 participated in this study that ran for two semesters.
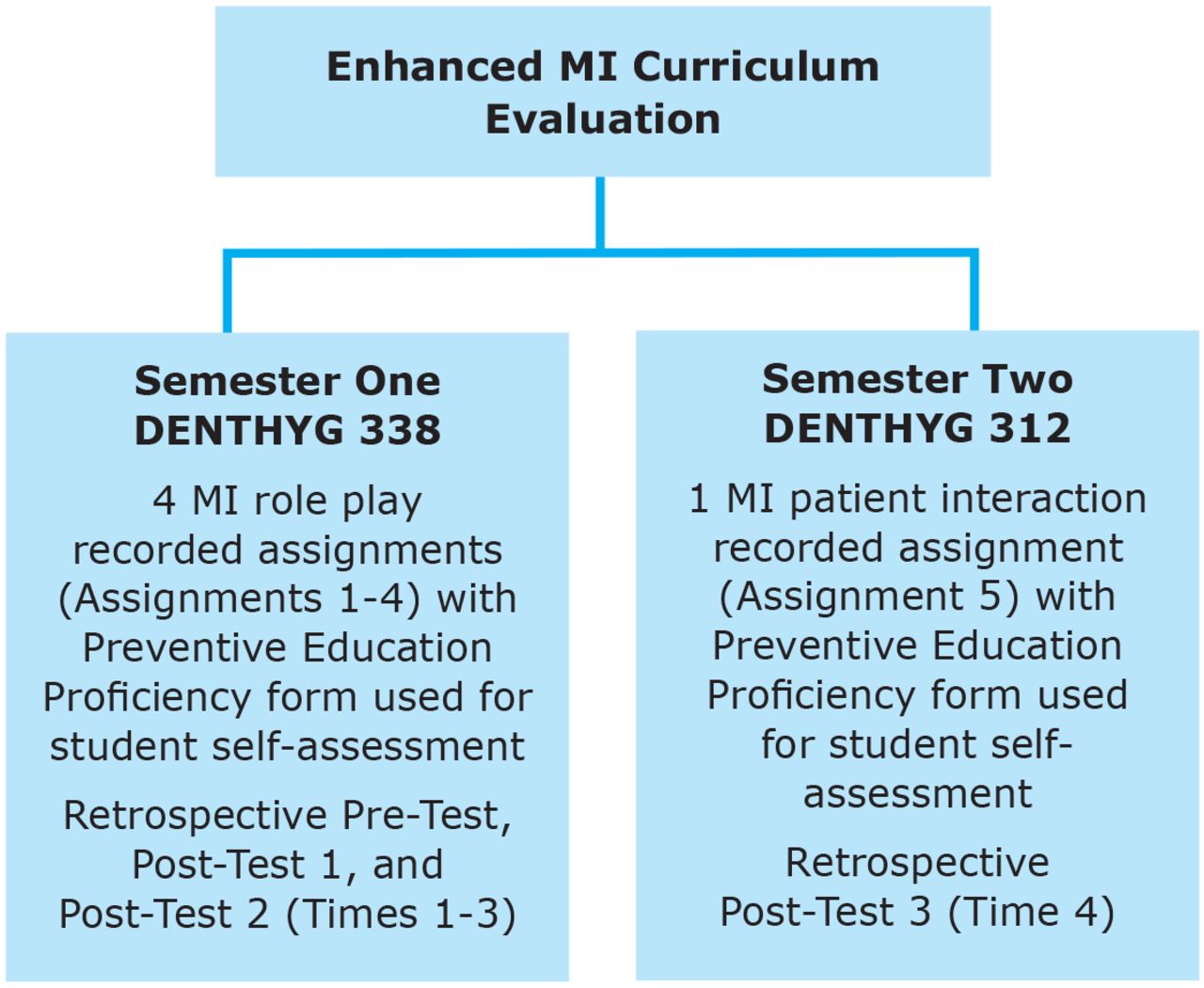
In the winter of 2013, the enhanced MI curriculum was launched. Prior to this, the students' exposure to MI consisted of a didactic session during the Health Education Methods course that also focused on the Stages of Change and Health Belief Models. There were no assignments integrating the application of MI. Figure 1 provides an overview of the enhanced MI curriculum evaluation timeline. During the first semester of the study, the students were enrolled in DENTHYG 338-Health Education Methods, a course that takes place during the second semester of the six semester dental hygiene program. The second semester of this study focused on the application of MI during patient care and was facilitated in DENTHYG 312-Clinical Dental Hygiene Seminar, a course that takes place during the third semester of the six semester dental hygiene program.

Enhanced MI Curriculum Evaluation Timeline
Semester One of the Study
During the 10 consecutive fifty-minute sessions of enhanced MI education and skill instruction presented in Health Education Methods, students were assigned to read MI literature, watch videos depicting scenarios of a MI counselor with a patient followed by group assessments of the interactions. Students were also required to complete four audio-recorded role-play assignments applying MI skills (Figure 1) The four evaluation instruments used in semester one of this study were adapted from those used by the University of Missouri-Kansas City Dental Hygiene Program during the assessment phase of their Motivational Interviewing curriculum. Modifications were completed in consultation with U-M's Center for Research on Learning and Teaching (CRLT). The modified instruments were then pilot-tested and the recommendations were incorporated.
In addition, the “Preventive Education Proficiency” form was utilized throughout this study. Both students and faculty used this proficiency form to assess audio-recorded MI role-playing interactions. Ten of the criteria focused on application of specific MI strategies such as asking permission, use of open-ended questions, reflection, affirmation, and summary. Two criteria asked students to self-assess their perceptions of the importance of using MI and confidence in applying MI techniques.
Students were required to complete four audio recordings. Assignment #1 focused on the students' application of open-ended questions, affirmations, reflective listening, and summarizing (OARS) principles. Assignments #2 and #3 were combined assessing additional MI strategies of complex reflection and eliciting change talk. Assignment #4 asked the dental hygiene student to assimilate and apply all MI strategies during a recorded interaction with an acquaintance.
A Retrospective Pre-Test was delivered to the Class of 2015 at the end of the 10 MI class sessions in DENTHYG 338 - Health Education Methods. This assessed the students' perceptions of how important they believed utilizing the MI counseling strategies were before the start of the course. This also assessed student confidence with using MI prior to DENTHYG 338. The MI strategies evaluated included: using open-ended questions, listening reflectively, making affirmations, summarizing, eliciting change talk, using the importance ruler, asking for elaboration, and enhancing self-efficacy. The Retrospective Pre-Test collected both importance and confidence responses using a Likert scale. Demographic information was also gathered.
Post-Test 1 was delivered to the Class of 2015 at the end of the 10 MI sessions in DENTHYG 338. Post-Test 1 assessed the students' perceptions of the importance of MI and their confidence in using it after completing the educational training. It utilized the same questions and Likert scale response options as the Retrospective Pre-Test as Post-Test 2. Post-Test 2 was delivered to the Class of 2015 on the last day of class, in order to measure the students' perceptions five weeks after the completion of the MI content in the course.
Demographic Information: Class of 2015 (n=22)
Semester Two of the Study
In the fall of 2013 during DENTHYG 312 - Clinical Dental Hygiene Seminar, the Class of 2015 completed a worksheet asking for a critical analysis of the change talk and commitment strategies as demonstrated in a video shown during class. In addition, the students participated in a 110-minute class session delivered by an expert in the area of MI. This presentation focused on eliciting change talk and setting the agenda for change with patients. During the second semester, students were also required to audio record an educational interaction with a patient in clinic (Assignment 5). Using the Preventive Education Proficiency form, students self-assessed their interaction, including their perceptions of importance of MI and their confidence in applying MI techniques. The team of faculty members also used this proficiency form to assess the students' recorded interactions and provide feedback.
Post-Test 3 was administered to the Class of 2015 at the end of the fall 2013 semester. The Post-Test 3 was used to again measure students' perceptions of the importance of MI and their confidence in using MI in delivering health education, with additional open-ended questions included.
Motivational Interviewing Definitions
Results
SPSS version 21 was utilized for data analysis. Descriptive statistics for the Class of 2015 are provided in Table I. Definitions of MI skills assessed “in this study adapted from Miller et al6 are summarized in Table II.
A Wilcoxon Signed Rank Test was used to compare the differences in average ranks between T1 (Retrospective Pre-Test) and T4 (Post-Test 3) for the importance and confidence questions at each of the designated time points for the Class of 2015 (Table III). Significance was set at (p<0.05). Statistically significant increases of importance were found between Time 1 and Time 4 in “open ended questions,” “making affirmations,” “summarizing,” “eliciting change talk,” and “enhancing self-efficacy.” No significant difference was found between Time 1 and Time 4 for “listening reflectively,” “using the importance ruler,” and “asking for elaboration.”
Confidence in “open ended questions,” “making affirmations,” “summarizing,” eliciting change talk,” “using the importance ruler,” “asking for elaboration,” and “enhancing self-efficacy” was found to be significant (p<0.05) over time. No significant changes were found for “listening reflectively.” Effect size was calculated using r-squared and ranged from .00 to .55.
Using the Preventive Education Proficiency form, self-perception of the importance of MI and confidence in applying MI skills was evaluated for the Class of 2015 using a Wilcoxon Signed Rank Test (Table IV). Change in students' importance and confidence scores over time was not statistically significant. Effect size was calculated using r-squared and ranged from .01 to .07.
Wilcoxon Signed Rank Test comparing T1 and T4 to assess mean differences in the Class of 2015
In Post-Test 3, in addition to the importance and confidence assessment, open ended questions were presented to the Class of 2015. Participants were questioned about successes using MI in patient care (Table V). Of the 22 study participants, 36% (n=8) found successes with “patient changes,” 27% (n=6) identified “improved communication” with patients with 14% (n=3) reporting “no patient behavior change.”
For the open-ended question related to MI challenges (Table VI), “patient issues” were identified as a challenge by 45% (n=10). Forty-one percent (n=9) perceived “time” as a challenge and 14% (n=3) of the responses fell into the theme labeled “other.”
Discussion
The Class of 2015 identified an increased perception of the importance of MI from Time 1 (Retrospective Pre-Test) to Time 4 (Post-Test 3) in five of the eight MI strategies. By Time 4 students had participated in four graded MI recording assignments in which faculty feedback was provided. In addition, they had two semesters in which MI had been integrated within didactic course work. Lastly, they had been providing clinical care to patients in both semesters. This increase in perception of importance associated with the majority of MI strategies may be attributed to students' involvement with the enhanced MI curriculum. This is similar to the results documented by DiMatteo et al., finding rigorous MI training was essential for skill development and requires practice and time.12 This finding is also consistent with studies documenting increased perception of importance of MI after students participated in curricula consisting of lectures, role-play activities, recordings including patient interactions, and faculty feedback.25-27,31
It is also important to note that from Time 1 to Time 4, student perceptions of the importance of using MI strategies did not always increase incrementally as noted in Table III. Time 4 was after an actual patient interaction recording. Actual application of MI strategies with patients appears to play a crucial role in training and education. Similar results were documented in a study by White et al., who found 83% of students reported that having MI in the curriculum had a positive impact on patient interactions and helped students be more comfortable discussing health behavior change with their patents.27
When the Class of 2015 was assessed on their perceptions of confidence in applying MI techniques, in seven of the eight MI techniques students identified a statistically significant increase from Time 1 to Time 4. Students gained valuable MI experience through classroom content, literature, watching videos depicting scenarios of a MI counselor with a patient, and recording role-play assignments along with a patient interaction. In all five assignments, students participated in self-assessment and were provided faculty feedback. This is consistent with previous studies indicating coaching with feedback had positive results in students' perceptions in their abilities to deliver healthcare education and counseling.25,27,30
The Class of 2015 used the Preventive Education Proficiency form to self-assess their perception of the importance of MI and their confidence in applying it at the completion of each of the five MI recording assignments over the two semesters. Overall importance and confidence increased however, the increase was not statistically significant. This could be due to the small, three point scale used, not allowing for enough variance in responses. Consideration should be given to revising the proficiency assessment to include a broader response scale.
In one of the open-ended data collection questions, students were asked about successes they had experienced using MI. Both improved communication and health behavior changes achieved by patients were identified as successes. This affirmed the ability for the students to utilize MI effectively with their patients, an important desired outcome of the enhanced MI curriculum. Miller and Rollnick documented those experiencing a positive perceived impact on patients achieved higher levels of competence and confidence.21
Wilcoxon Signed Rant Test comparing the mean differences in the Class of 2015's self-assessment of importance and confidence between T1 and T4 and T1 and T5, using the Preventive Education Proficiency form
MI Successes
MI Challenges
Challenges reported with MI included not having enough time in clinic to complete the proficiency recording with a patient, which aligns with similar feelings of health practitioners working in the field.32 Given that the utilization of multiple MI strategies in one sitting can take a significant amount of time, utilizing brief motivational interviewing may be more appropriate with previous studies demonstrating this to be successful in health care settings.13,14,33
This study had limitations; the small sample size and the lack of a control group. Development of interpersonal communication skills should involve practice and be closely evaluated.9,10 Training research indicates that proficiency in MI is not readily developed through self-study or by attending a workshop, but typically requires practice with feedback and coaching over time.11,20 It is recommended that the U-M Dental Hygiene Program continue this study longitudinally so the outcomes from the Class of 2015 can be determined following three full years of the enhanced MI curriculum.
Conclusion
This study found students' perceptions of the importance of MI and their confidence in applying MI strategies increased over time. Students identified important successes when applying MI and also identified realistic challenges in the process. These findings supported that the enhanced curriculum had a positive outcome on students' ability to learn important MI concepts and apply these in health behavior change interactions. Future research should focus on measuring student performance related to patient health behavior change outcomes longitudinally. In addition, additional studies should concentrate on faculty feedback and coaching calibration.
Acknowledgements
The authors wish to thank Kimberly Bray, RDH, MS and Delwyn Catley, PhD, from the University of Missouri-Kansas City, for their guidance during this project. Gratitude is also extended to Dina Korte, RDH, MS and Giselle Kolenic, BA, MA, from the University of Michigan, for direction, dedication, and support.
Footnotes
Angela Mills, RDH, BSDH, MS, is a 2014 graduate of the Master of Science in Dental Hygiene Program, University of Michigan School of Dentistry, Ann Arbor, MI, and an adjunct faculty member at Oakland Community College, Highland Lakes, MI.
Wendy E. Kerschbaum, RDH, MA, MPH, is an Associate Professor Emerita; Philip S. Richards, DDS, MS, is a Clinical Professor; Janet S. Kinney RDH, MS, is Director of Dental Hygiene and a Clinical Associate Professor; and Anne E. Gwozdek, RDH, BA, MA, is a retired Clinical Assistant Professor; all in the Department of Periodontics and Oral Medicine, University of Michigan School of Dentistry, Ann Arbor, MI. Gail A. Czarnecki, DDS, is a pediatric dentist in private practice in Arlington Heights, IL.
This manuscript supports the NDHRA priority area, Client level: Oral Health Care (new therapies and modalities).
- Copyright © 2017 The American Dental Hygienists’ Association





{kind=link}