



Abstract
Purpose: Progress in the dental hygiene discipline is predicated on the development of a community of scholars with a dental hygiene scholarly identity who explore questions central to the art and science of dental hygiene and in doing so create conceptual models to expand the discipline's structural hierarchy of knowledge. Graduate dental hygiene education is challenged to develop programs that stimulate and nurture dental hygiene scholars as well as scientists. The need for the development of dental hygiene doctoral education is critical to strengthening our discipline's scholarly identity.
The authors explore the tyranny of the “Queen-Bee” and the paralyzing nature of the “Imposter Syndrome,” as pathologic non-productive behavior patterns that create roadblocks not only for the individual to move forward, but also for the discipline as a whole. Recognizing and eliminating these maladaptive syndromes will empower the individual as well as strengthen the collective to build a strong dental hygiene scholarly identity. The significance of dynamic “Follower-ship” as an often undervalued concept is offered as an antidote to overcome roadblocks and energize the collective's value of a scholarly identity for dental hygiene.
- scholarly identity
- graduate dental hygiene education
- dental hygienists
- doctoral dental hygiene education
- imposter phenomenon
- queen bee syndrome
- follower-ship
Introduction
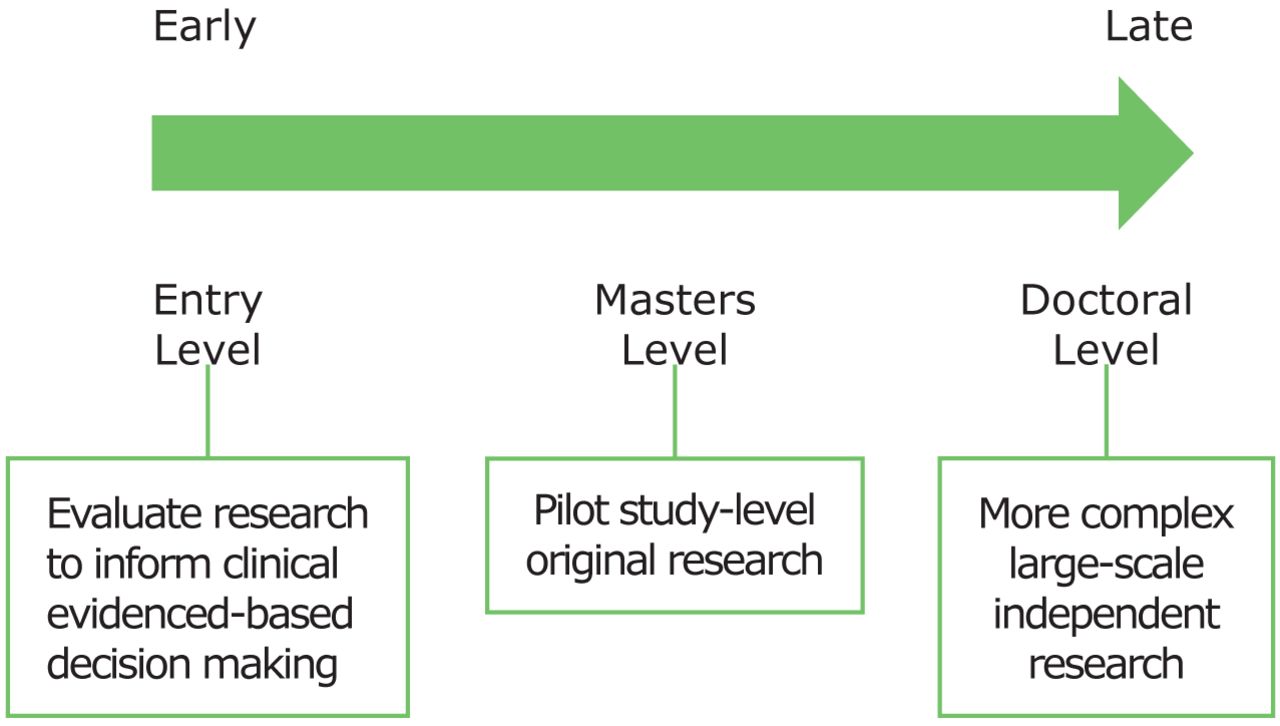
Scholarship development in dental hygiene is a very broad concept, but it can be thought of as existing on a continuum (Figure 1). At one end of the continuum scholarship begins in entry-level dental hygiene programs where students learn to review and evaluate the literature to inform clinical evidence-based decision-making. This continuum progresses to higher levels of scholarship in research-oriented dental hygiene master's degree programs where learners conduct pilot study-level original research, and in research-oriented dental hygiene doctoral degree programs that require more complex, large-scale original independent research.1 For the purpose of this paper, the term scholarship will refer to that aspect of the continuum that relates to conducting original research.
In most disciplines, the doctoral degree is the terminal degree preparing scholars to conduct rigorous discipline-specific research.2 Although the first dental hygiene doctoral program was established in 2013 at Namseoul University in South Korea, and there is one such program on the drawing board in the U.S. at Idaho State University, much of the responsibility for dental hygiene's higher level scholarship development falls to the dental hygiene master degree programs throughout the world.3 Indeed, graduate learners enrolled in dental hygiene research-oriented master degree programs develop competencies related to the research process needed for the development of dental hygiene scientists. However, to further develop the dental hygiene discipline to promote the public's oral health, dental hygiene scholars are needed in addition to dental hygiene scientists. An underlying theme of this paper is that there is a difference between a dental hygiene scientist and a dental hygiene scholar.
Scientists systematically pursue answers to questions related to substantive areas of some discipline. Scholars, on the other hand, not only are research scientists, but they also have a dedicated and passionate commitment to how their science relates to their discipline's mission, its values and its effects on humanity. In this context, scholars have a sense of the discipline's history and have a life-long commitment to the development of the discipline's knowledge base through focused research programs.1,4,5 For example, many dental hygiene scientists often focus on isolated questions that may or may not be directly related to the dental hygiene discipline. Thus, we have scientists who are dental hygienists, rather than dental hygiene scientists who also are dental hygiene scholars. Although this nuance may appear to be trivial, it is an essential distinction when it comes to the advancement of the dental hygiene discipline as it moves through its scholarship development process. Therefore, the purpose of this paper is to:
Define the dental hygiene scholarly identity
Discuss the importance of the dental hygiene scholarly identity to advancing the dental hygiene discipline and its structural hierarchy of knowledge to promote the public's oral health
Introduce potential roadblocks to developing the dental hygiene scholarly identity and strategies to overcome them
Introduce the concept of follower-ship in developing a community of dental hygiene researchers with a dental hygiene scholarly identity
The Scholarly Identity
Dental hygiene researchers who have a scholarly identity are dental hygiene scientists who:
Envision the dental hygiene discipline as a whole
Conceptualize theory central to the discipline as the basis for further knowledge development
Develop and test conceptual models from the dental hygiene perspective
Incorporate the norms and values of the dental hygiene practitioners
Ask and answer research questions central to the discipline while reaching across disciplines
Focus on dental hygiene research priorities6
See their research questions as part of the discipline's whole
Have a commitment to the discipline's knowledge development
Have a sense of belonging to a dental hygiene scholarly group
Welcome philosophical debate about the discipline
Dedicate themselves to mentoring other dental hygiene scholars
Apply knowledge of existing dental hygiene theories to their research questions
Like other scientists, dental hygiene scientists with a dental hygiene scholarly identity also:
Apply knowledge of research design, methodologies and statistics to guide the scientific process
Use evidence to support their viewpoint
Report one's own results in the context of those of others in the field as well as those in other disciplines
Disseminate their research findings through scientific publication1
Dental hygiene masters programs are challenged to do the above within a limited timeframe of 1 to 2 years. Nevertheless, developing a scholarly identity and community among master degree-level dental hygiene learners is a first step toward making progress in developing the dental hygiene discipline. Dental hygiene doctoral programs are needed to complete the journey

Continuum of Dental Hygiene Scholarship Development
So, how does the dental hygiene scholarly identity relate to the dental hygiene discipline's Structural Hierarchy of Knowledge?
The Structural Hierarchy of Knowledge
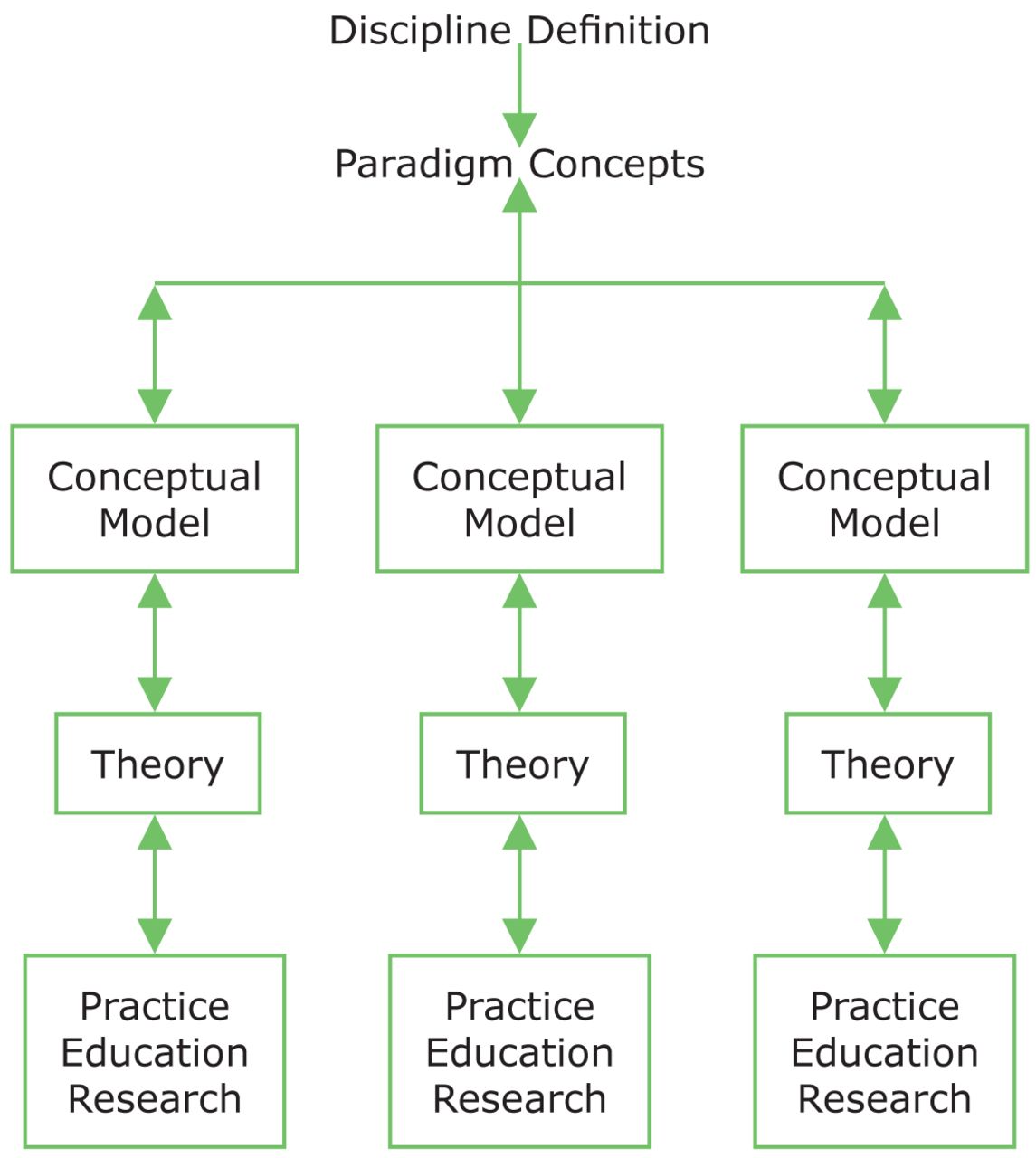
Most disciplines have a formal metaparadigm or Structural Hierarchy of Knowledge that is a widely accepted worldview of the discipline. Figure 2 represents a generic Structural Hierarchy of Knowledge for any discipline that is composed of the definition of the discipline, its major paradigm concepts the discipline has selected for study and conceptual models.12,13 The paradigm concepts are established by the discipline, specify the discipline's unique perspective and are the first level of distinction between similar disciplines. Although the paradigm concepts are not subject to change by scholars, they are used by scholars to develop conceptual models. Conceptual models are also known as schools of thought. Each school of thought (i.e., conceptual model) relates to some theory and is designed to be tested by scholars to then either accept or reject the school of thought. A conceptual model (i.e., school of thought) shapes the direction and methods of the practitioners, educators and researchers who subscribe to that particular school of thought.
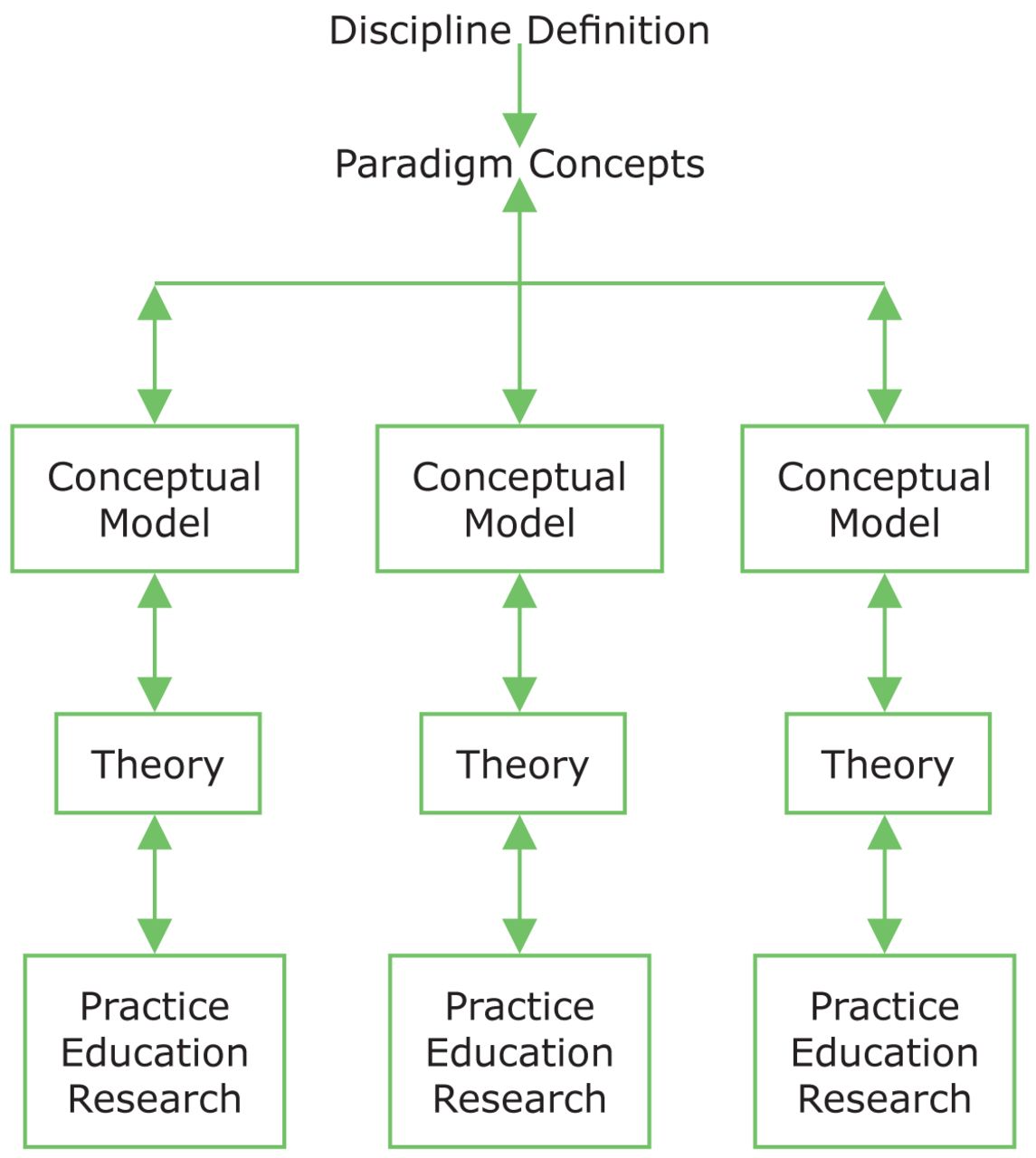
Generic Diagram of the Structural Hierarchy of Knowledge for All Disciplines
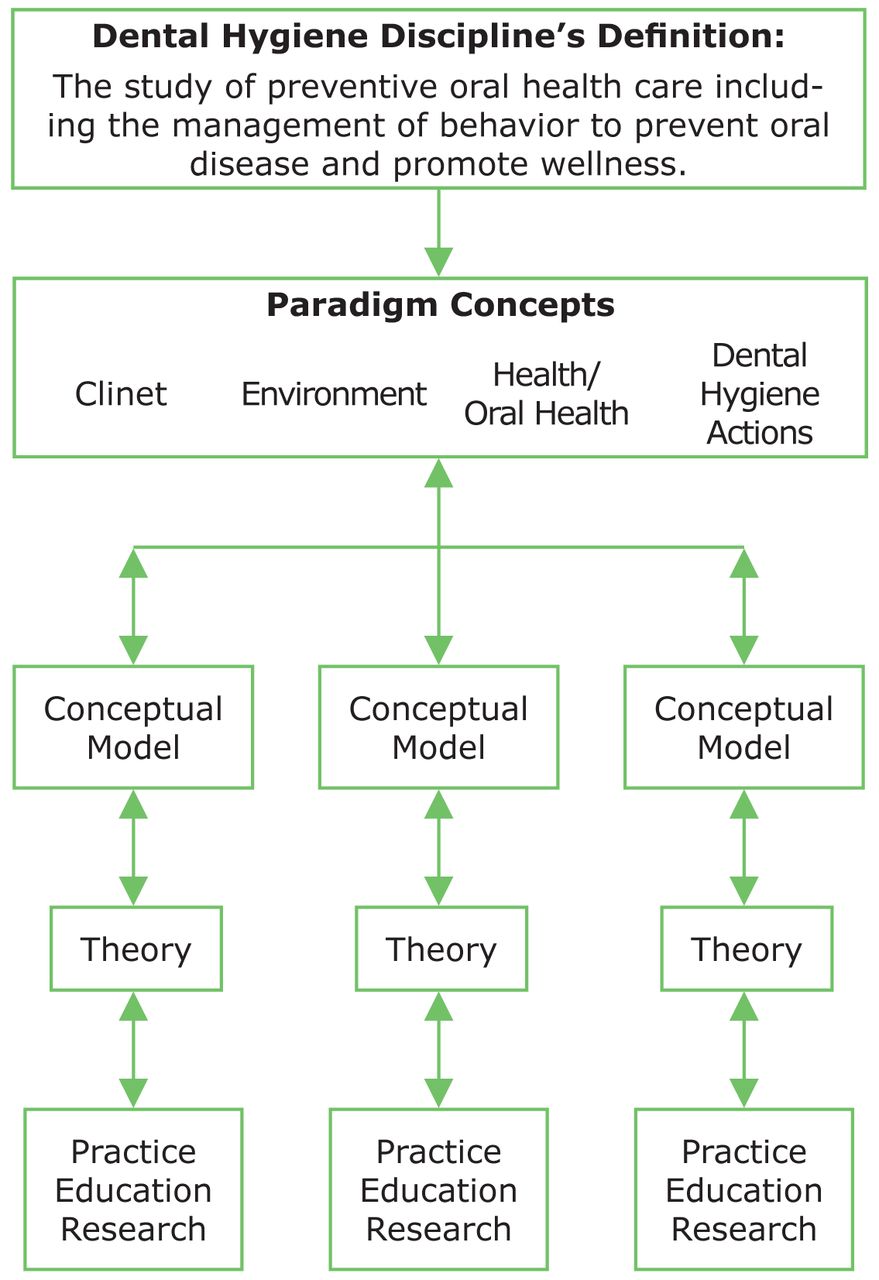
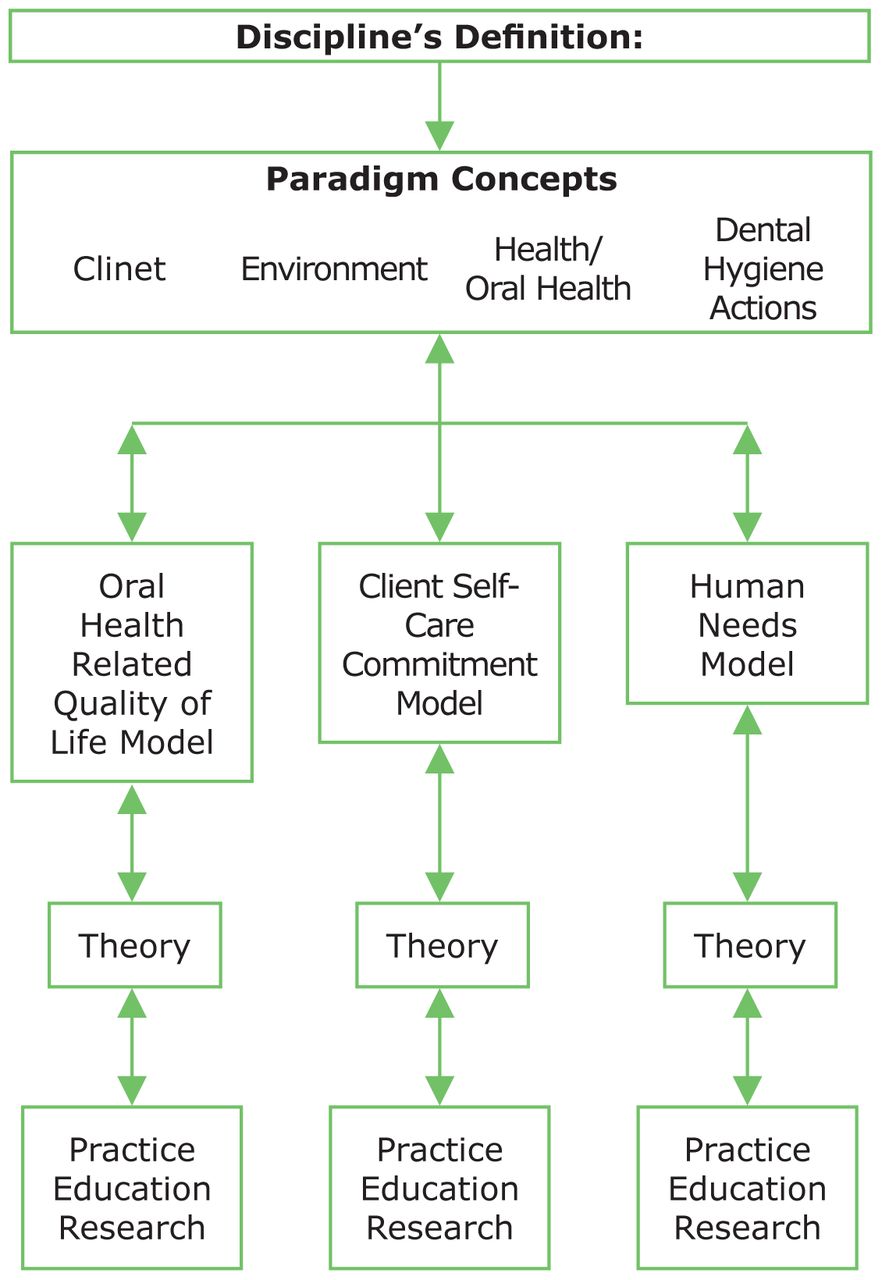
Figure 3 illustrates the Structural Hierarchy of Knowledge for the dental hygiene discipline.12-14 This hierarchy was approved by the ADHA House of Delegates in 1995,14 and consists of:
The definition of the discipline
Paradigm concepts
Global definitions of the paradigm concepts
Conceptual models (Open to innovative development by dental hygiene scholars as theory-based schools of thought)
The details of these components of dental hygiene's Structural Hierarchy of Knowledge are reviewed below.
Component #1: The Definition of dental hygiene. Dental hygiene as a discipline is defined as “the study of preventive oral healthcare including the management of behaviors to prevent oral disease and to promote health.”14 This definition is unique because it focuses on oral disease prevention and health promotion from the dental hygiene perspective. That perspective promotes clients who are empowered to perform oral self-care, chronic oral conditions that are improved, quality of life that is enhanced and oral disease prevention with associated lower oral health care costsl.11

Dental Hygiene Discipline's Structural Hierarchy of Knowledge
Note the phrase “the study of” in the definition because that is what all disciplines do - they study important concepts that contribute to the discipline's body of knowledge to inform practice and to enhance the public's oral health.13,14
Component #2: Dental hygiene's Paradigm Concepts. Paradigm Concepts are the second component of any discipline's hierarchy of knowledge. The 4 concepts selected for study by the dental hygiene discipline are:11,12
The Client
The Environment
Health/Oral Health
Dental Hygiene Actions
Component #3: Global Definitions of Each Paradigm Concept.13,14 A discipline's paradigm concepts always are defined very broadly to allow for the development of conceptual models about the concepts that are defined by specific theories.15 Therefore, the concept of the Client, has been defined by the ADHA, as “the recipient of dental hygiene actions who may be an individual, a family, a community, or a particular group.” The term “Client” was selected as a paradigm concept, rather than the term “Patient,” because the term “Client” is:
Broad, not limited to an individual
Implies wellness rather than illness
Implies an active rather than a passive relationship with the provider
In contrast, the term “Patient” connotes:
An individual
Control by the health care provider
A dependent passive recipient
The need for therapy only
A focus on biological problems with potential neglect of the individual's psychological, sociocultural and spiritual wellness
Although the term “Patient” is a correct clinical term widely used by dental hygienists to refer to the recipients of their care, it was not selected as a Paradigm Concept because of its more restrictive focus than that of the term “Client.”
The concept of the Environment is defined as the milieu in which the client and dental hygienist find themselves.14 This concept includes dimensions such as socio-ethno-cultural, economic, political and educational factors that act as either barriers or facilitators to health, oral health and dental hygiene actions.
The concept of Health/Oral Health is defined as the client's state of well-being that exists on a continuum from maximum wellness to maximum illness.14 Oral health and overall health are interrelated because each influences the other.
The concept of Dental Hygiene Actions is defined as the interventions provided by a dental hygienist on behalf of, or in conjunction with, the client to promote oral wellness and prevent oral disease.14 These 4 global paradigm concepts central to the discipline of dental hygiene have been and continue to be further defined and expanded into various conceptual models that drive dental hygiene education, research and practice.
It must be recognized that early in its inception, dental hygiene drew heavily on knowledge from other disciplines such as dentistry, nursing, education and psychology.15-18 However, over the last 100 years, dental hygiene scholars have developed many of these borrowed concepts into new conceptual models from the perspective of dental hygiene making them sufficiently distinct.19-21
Component #4: Conceptual Models. Conceptual models can be thought of as schools of thought. Just as in the discipline of psychology there are different schools of thought such as the Freudian school, or the Jungian school, so too in dental hygiene there are different schools of thought that affect research, education and practice. There can be as many conceptual models as there are scholars who can create them. Figure 4 shows 3 examples of dental hygiene conceptual models reported in the literature and each describes a unique process of care that is distinct for dental hygiene.19-21
The Oral Health-Related Quality of Life Conceptual Model is based on the premise that a satisfactory level of oral health, comfort and function, as defined by the client, is an integral component of general health.19 This model recognizes the oral cavity is a primary source of sensory input, and social discourse and functioning at all phases of life. It measures health and disease along a continuum that encompasses 6 domains of health, proposes a dynamic relationship among the domains and client characteristics, and serves as a foundation for the dental hygiene process of care (Table I).
The Client Self-Care Commitment Model is based on the premise that effectively involving clients as co-therapists in their oral health decisions, enhances motivation, commitment and compliance with oral self-care.20 The model proposes 5 domains to encourage active client self-involvement in oral health maintenance. It also proposes that there is a relationship among the domains and the client and dental hygienist interaction that empower clients to make decisions to enhance their own health through commitment and compliance (Table I).
The Human Needs Conceptual Model is based on the premise that human behavior is motivated by human need fulfillment and defines the paradigm concepts in terms of human need theory.21 This model proposes that there are 8 human needs related to dental hygiene care that form the basis of the dental hygiene process of care: assessing the 8 human needs, diagnosing deficits, setting goals and dental hygiene interventions, implementing, evaluating, and documenting the extent goals are met (Table I).
It is important to note that there are other conceptual models being offered by scholars beyond the above examples that require testing for the on-going evolution of dental hygiene's body of knowledge and recognition of dental hygiene as a distinct profession.
For each conceptual model (i.e., school of thought), research questions are asked to test the model and findings contribute to the dental hygiene discipline's body of knowledge to guide dental hygiene practice. The problem, however, is that none of these models have been sufficiently tested in the realities of dental hygiene practice settings to determine their effects on oral health and the quality of dental hygiene care.15,22-25 We need to ask the question, Why?
As we ponder this question, let us consider that Einstein once said: “No problem can be solved from the same level of consciousness that created it.”26 The first step in solving a problem is to define the problem. It makes one wonder: Could it be that many of our dental hygiene educators, researchers and clinicians are not fully aware of the discipline's hierarchy of knowledge and of the importance of developing a scholarly identity related to it? Could it be that there are unconscious, maladaptive behavior patterns among dental hygienists that create roadblocks to moving the discipline forward? And, if these threats are real, then what can be done to counteract them? To challenge our thinking about these questions and to provide some essential information needed for possible answers, a discussion of potential roadblocks to developing a dental hygiene scholarly identity follows.
Potential Roadblocks to Developing a Scholarly Identity
Although in-roads have been made towards gender balance, to date dental hygiene remains predominantly a female profession.27 Therefore, it is important to recognize 2 prevalent maladaptive behavior patterns prevalent among women who have succeeded in their careers that may be potential roadblocks to developing a dental hygiene scholarly identity. These behaviors are known as the “Imposter Phenomenon” and the “Queen Bee Syndrome.”28 The central psychological feature of both the Imposter and the Queen Bee is a distorted self-image. Although it is important to recognize and explore other dysfunctions that also may hold back the on-going evolution of the profession, only the Imposter Phenomenon and the Queen Bee Syndrome are discussed in this paper as described below.
The Imposter Phenomenon
The Imposter Phenomenon, prevalent among high-achieving women, was first described in 1978 as the perception of oneself as having an “intellectual phoniness.”29 Although studies report that men experience the phenomenon as frequently as women, the Imposter Phenomenon's characteristics have a more deleterious effect upon a woman's career.29 Women who experience the impostor phenomenon believe that, despite outstanding academic and professional accomplishments, they really are incompetent, and that anyone who believes otherwise has been fooled.29,30 Symptoms they experience are anxiety, self-doubt, inability to accept positive feedback, fear of failure and guilt about success undermine their ability to function at their highest level. The Imposter Phenomenon also can be applied to a group.31

Dental Hygiene Discipline's Structural Hierarchy of Knowledge with 3 Examples of Dental Hygiene Conceptual Models
One explanation for a higher prevalence of this disorder among women than men is that society sometimes imposes contradictory values upon children, so that what is socially desirable in men may be different from what is socially desirable in women.29 Contrary to the male perspective, for a woman, claiming power may be accompanied by fears of selfishness, destructiveness and abandonment. This negative perception is an image that few women can bear; consequently, some women are more comfortable feeling inadequate than feeling successful. The Imposter Phenomenon becomes a defense mechanism that allows these women to deal with ambivalence about their successes by keeping their achievements out of self-awareness.29 For example, a high achieving dental hygiene leader who suffers from the Imposter Phenomenon may not be able to find her voice to defend her support of a dental hygiene doctoral program proposal, or of a new conceptual model unique to dental hygiene practice when confronted by skeptical questions from members of a more dominant group that the dental hygienist perceives as having greater prestige, power and status. This situation is compounded in academic settings, where dental hygiene leaders may be rewarded for being marginal and taking on the characteristics of the dominant group, rather than advocating for the values and advancement of the subordinate group.
Examples of 3 Dental Hygiene Conceptual Models That Describe a Unique Process of Care that is Distinct for Dental Hygiene
In such situations where we find ourselves having to defend a foreign idea to a more dominant group, it is important to anticipate the potential for the Imposter Phenomenon to derail success.32 Conducting a mock presentation to practice responding to difficult questions before presenting the proposal is a suggested preventive strategy. Employing the counsel of the “5 P's” is helpful in that “Proper Preparation Prevents Poor Performance.”33
Most importantly, to counteract the potential for the Imposter Phenomenon, each of us must realistically assess our traits and celebrate our individual strengths and successes while forgiving our imperfections and mistakes.29 The goal is that when we find ourselves in a position of acceptance by the more dominant culture, we will be self-aware, confident in our achievements, clear in our dental hygiene identity and able to overcome Imposter Phenomenon symptoms if they arise. Being aware of the Imposter Phenomenon allows one to establish control driven by inner strength and commitment, not fear.32 A good cognitive strategy to cope with the self-doubt characteristic of the Imposter Phenomenon is for an individual to re-direct her focus from herself and her own shortcomings to that of the needs of the task at hand and of being of service to others.32 It is normal to have fear, but it is important not to allow fear to drive our decisions about taking action when opportunity presents itself.34
The Queen Bee Syndrome
Another threat to success in achieving a dental hygiene scholarly identity and in establishing dental hygiene doctoral programs is the Queen Bee Syndrome.35 The Queen Bee Syndrome, first defined in 1974, describes a woman in a position of authority who views or treats subordinates more critically if they are female. The “Queen Bee” is one who has succeeded in her career, but refuses to help other women do the same. This condition has been documented by several studies.36 The Queen Bee protects her status by developing behaviors that are entrenched with self-centered motivation. She shuns subordinates, avoids competition and associates with the male-dominated management group rather than female peers.36 Unlike other types of alpha females in a position of power who engage in collaboration and compromise, the Queen Bee lacks compassion and feels the need to aggressively destroy other females who are perceived as competition to her and potential threats to her hard-earned elite position.35
Like the Imposter Phenomenon, the Queen Bee Syndrome is a defense mechanism. By assuming Queen Bee behaviors, she copes with the conflicting demands of her professional role and the role women have traditionally held in the family. She operates on a double standard; what is right for her is not always right for other women.28 The tragedy is that these talented but maladaptive women leaders often have the opportunity to support the goals of female groups, but frequently may not.28 Instead of being supportive, the Queen Bee becomes a barrier to power and achievement for other women, especially if they are members of a subordinate group from which the Queen Bee originally was a member.28,37
Many academic dental hygienists have considerable influence on academic decision-making within their academic institutions about whether or not to develop innovative academic programs such as dental hygiene doctoral degree programs. Although it is important to be clear that most high achieving dental hygienists who advance in the academic system are not Queen Bees, it is critical to recognize a Queen Bee when one is encountered and not be blind-sided because of trusting naiveté. Instead, once we recognize a Queen Bee who has the power to influence others negatively regarding any proposal for which we seek approval on behalf of the dental hygiene discipline, the best practice is to seek the endorsement of someone else in the dominant culture that has more prestige than she before seeking her support. Even then, she may not become an advocate, but she will keep her aggression at bay to comply with her superiors. The Queen Bee always is controlled by forces outside herself that have greater prestige, power and status.35
Certainly, all high achieving women can fall prey to becoming a Queen Bee if they are unaware of this syndrome and its adverse consequences.31 Some useful strategies to minimize the effect of a Queen Bee are to:38
Stop giving away personal power by thinking or acting like a victim - instead, look for alternative pathways to get what is needed accomplished
Focus on objectives and maintain dignity and integrity while striving to do what is best for the group
Find a mentor who not only is successful in human relationships, but also is someone with whom you are confident you can share intimate details
Indeed, dental hygienists must engage in self-reflective processes and look beyond the role of the Queen Bee for other leadership styles that will complement not only the needs of the leader, but also those of the dental hygiene profession and its clients. Leadership behaviors needed may lie in the concept of “Followership”discussed below.39
Followership
Taking action to be a more effective follower is a potential antidote to the roadblocks created by the Imposter and Queen Bee syndromes. But what do we mean by Followership? According to Followership Theory, there are 5 follower roles that are determined by levels of activity and critical thinking.39,40 These roles are: sheep, yes people, alienated followers, survivors and effective followers. Taking action to develop and adopt effective follower characteristics in dental hygiene is key to counteracting the destructive results of maladaptive behavior patterns of leaders and in developing a “scholarly identity” to move the discipline forward. Effective Followers are active rather than passive. They can and should initiate change and engage in problem-solving and ethical behavior. Followership theory describes the role of “Followership” as a component of leadership,41 and views leaders and followers as “two sides of one process, two parts of a whole.”42 Effective follower's work hard to overcome the Imposter Syndrome. They actively listen without interrupting, ask a lot of questions, display an attitude of service by looking for opportunities to share their expertise, focus on solution when there is a difference of opinion, and are inclusive sharing not only the workload but also the recognition.40 When a Queen Bee is identified, effective followers take responsibility for using alternative paths to achieving the group's goals. In doing so, they often emerge as alternative leaders when the situation demands it. In other words, passive people are not followers.43 Rost goes as far to say that effective “followers do not do followership, they do leadership.”44
Thus, the term Followership honors and recognizes the crucial role Followers play in organizational life. The term Followership recognizes that followers and leaders are dynamic roles that can be exchanged, and that performance challenges, not position, determines when one follows and when one leads.40,41 Effective followership prepares one to be an effective leader, as demonstrated in the video clip entitled the Leadership Lessons and the Dancing Guy.38 This video illustrates the importance of followership to leadership and that being a “first follower” is an under-appreciated form of leadership.45,46 Dental hygiene needs to get past an elitist view of leadership that supports the Queen Bee, and a passive conformist view of followership that coincides with the Imposter Phenomenon. Much of a leader's success depends on effective followers and both roles deserve equal weight.44
Conclusion
There is a critical need for a community of passionate dental hygiene researchers with a dental hygiene scholarly identity to ask and answer questions related to the discipline's whole while reaching across disciplines for assistance. These dental hygiene scholars are essential for the advancement of the dental hygiene discipline's knowledge base to promote the public's oral health. This paper has reviewed 3 dental hygiene conceptual models, however, there can be as many conceptual models and frameworks as there are scholars who can develop them. As more conceptual models evolve beyond what is offered in this paper, they should be tested and examined as well.
Recognizing the potential for the Imposter Phenomenon and the Queen Bee Syndrome to undermine dental hygienists' ability to function at their highest level, will empower the individual as well as strengthen the dental hygiene collective. Future research is needed to study these and other dysfunctions as impediments to achieving a professional scholarly identity. Such strategies as effective followership also are needed to take action to build a strong dental hygiene scholarly identity. In addition, the development of dental hygiene doctoral programs is critical to nurturing the dental hygiene scholarly identity, and to participate fully in interdisciplinary research. Moreover, doctoral dental hygiene education will expand the profession's opportunity to engage in health care workforce discussions, the development of innovation in educational programs, and in general to help address the oral health challenges of our nation and elsewhere.23
Acknowledgments
The authors would like to thank Joanna Hill, MSDH Program Administrator for her editorial support.
Footnotes
Margaret Walsh, RDH, MA, MS, EdD, was a Professor Emerita and former Director of the Master of Science Degree Program in Dental Hygiene, Department of Preventive and Restorative Dental Sciences, University of California, San Francisco. Elena Ortega, RDH, MS, is the interim Director of the Master of Science Degree Program in Dental Hygiene, Department of Preventive and Restorative Dental Sciences, University of California, San Francisco. Barbara Heckman, RDH, MS, is a Health Sciences Associate Clinical Professor, MS in Dental Hygiene Program, Department of Preventive and Restorative Dental Sciences, University of California, San Francisco.
This study supports the NDHRA priority area, Professional Education and Development: Identify the factors that affect recruitment and retention of faculty.
- Copyright © 2016 The American Dental Hygienists’ Association





{kind=link}
{kind=link}
{kind=link}
{kind=link}