



Abstract
Purpose: Oregon allows dental hygienists to provide services without the supervision of a dentist if they hold an expanded practice permit (EPP). This study surveyed practicing and non-practicing EPP holders with the purpose of assessing perceived barriers to practicing independently and better educating students to begin independent practice upon graduation.
Methods: A survey was developed, approved by the institutional review board and pilot tested with current Expanded Practice Dental Hygienists (EPDHs). A list of EPDHs was obtained from the Oregon State Dental Board, and 181 surveys were mailed in November 2011.
Results: The response rate was 39% (n=71). Data from this study indicate a large number of new EPP holders, with 62% (n=41) holding their permit for 3 years or less, but only 41% (n=29) of respondents are actually providing care in a setting requiring an EPP. Responding practicing EPDHs reported barriers including: challenges with insurance reimbursement, lack of knowledge/acceptance, equipment cost/maintenance, difficulty obtaining a collaborative agreement/cooperating facility, advertising and inability to make a living wage. Responding non-practicing EPDHs reported barriers including: currently working in another setting, lack of business knowledge, time, start-up cost, inability to make a living wage, lack of opportunity, reimbursement difficulties and lack of experience.
Conclusion: Perceived barriers to practicing independently differ between those practicing utilizing their EPP and those not practicing. Ways to eliminate barriers for both practicing and non-practicing EPDHs should be explored. There is potential to reduce the barriers to independent practice through curricular changes, public health partnerships among EPDHs, and new health care systems that specifically address barriers found through this study.
- dental Hygiene extended practice permits
- access to oral health care
- direct access
- independent practice
- dental hygiene
- limited access
- expanded practice
Introduction
It has been over a decade since the U.S. Surgeon General issued a report stating that oral health is an essential component of overall health.1 Yet getting access for all populations to quality dental care is still a major concern - reports consistently document a shortage of dentists in rural and inner city communities, and marginalized populations that do not receive regular dental care, with 45 million people living in these areas.2 It has been proposed that expanding the role of dental hygienists is one way to increase access to care for the underserved.3,4
In order to expand opportunities for dental hygienists and improve access to care, some states and countries utilize a mid-level practitioner in the dental field. Examples include the Dental Health Aide Therapist in New Zealand, the Dental Health Aide Therapist in Alaska, and the Dental Therapist, as well as the Advanced Dental Therapist, in Minnesota. Mid-level providers can perform a wide range of clinical services such as basic restorative procedures and extractions, in addition to the traditional repertoire of dental hygiene services.5-7 While most states do not utilize a mid-level practitioner, over the past decade many states have expanded the legal scope of practice of dental hygienists.8 Currently, 35 states allow dental hygienists to initiate patient care in a setting outside of the private dental office without the presence of a dentist in what the American Dental Hygienists' Association (ADHA) defines as direct access states.9 The term direct access means that the dental hygienist can initiate treatment based on his or her assessment of patients' needs without the specific authorization of a dentist, treat patients without the presence of a dentist and can maintain a provider-patient relationship.10
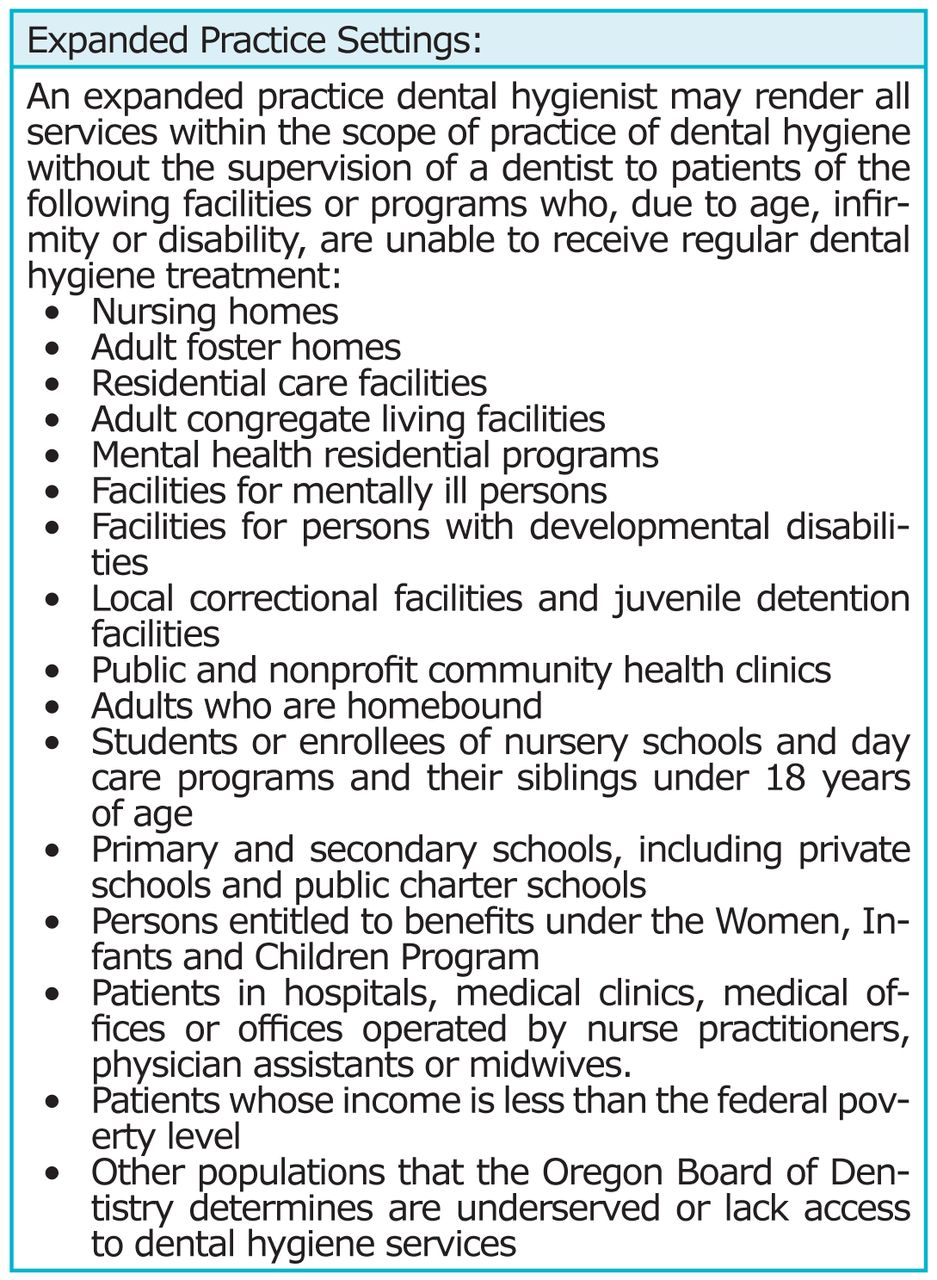
In the state of Oregon a mid-level practitioner does not exist, however, direct access does. Legislation was passed in 1997 to allow dental hygienists to attain a limited access permit.11 Legislation was later passed in 2012 renaming the limited access permit to the expanded practice permit (EPP). The EPP enables dental hygienists to provide a variety of dental hygiene services, without the supervision of a dentist, for “limited access” regions or populations (Figure 1). Expanded practice dental hygienists (EPDHs) are required to refer patients to a dentist at least once annually for examination and treatment of active dental disease. EPDHs do not need a collaborative agreement with a dentist to initiate dental hygiene care for patient populations that qualify as having limited access to care. If an EPDH wishes to perform additional services, such as providing local anesthesia, placing temporary restorations, and prescription of prophylactic antibiotics and non-steroidal anti-inflammatory drugs (NSAIDs) (which are included in the law), they must have a collaborative agreement with a dentist to provide those additional services. Many EPDHs work as employees in non-dental settings like nursing homes or schools. Other EPDHs become private business owners. One pathway to obtain an EPP is to have 2,500 hours of clinical dental hygiene practice and complete 40 hours of continuing education of the individual's choosing. An additional pathway to obtaining an EPP credential is to complete a course of study approved by the Oregon State Dental Board and have at least 500 hours of dental hygiene practice on patients in “limited access” settings while under the direct supervision of dental or dental hygiene faculty of an accredited program (Figure 2). Until October 2010, there were no board-approved courses of study.12 At that time, the Oregon Legislature passed a bill allowing applicants to apply hours spent during training (dental hygiene school) with patients in underserved or limited access settings to their 500-hour quota. Thus, under recently amended legislation, students are potentially able to attain an EPP upon graduation.
The goal of recent legislative changes is to facilitate a significant improvement in the access to care crisis in Oregon. To date, however, limited information exists regarding the impact of expanded practice dental hygienists as well as the barriers faced in pursuing expanded practice. The only study to date of Oregon EPDHs was conducted in 2005 by Battrell et al.13 This qualitative study included 7 Oregon EPDHs as well as 2 dentists. Participants perceived a need for expansion of scope of education to prepare for independent practice and called for additional curricular experiences to include coursework on organizational structure, billing, coding, prescription writing and the public health delivery system. One dental hygiene school in Oregon, Pacific University, has implemented curricular changes aimed at decreasing the barriers to entering independent practice, but the influence these courses have on the likelihood of graduates pursuing independent practice has not been measured. The perceived barriers to date have also not been formally measured.
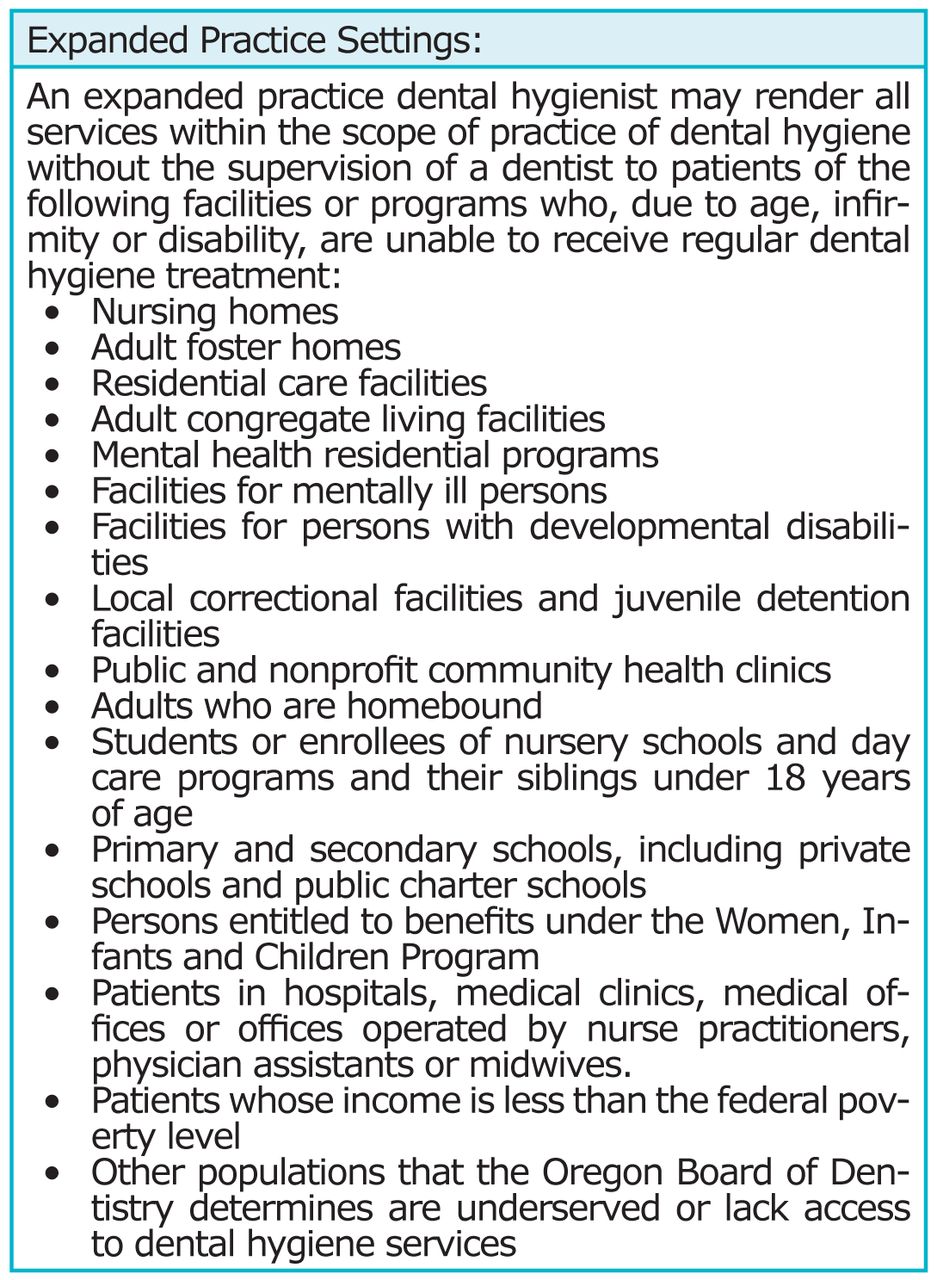
Practice Settings in Which EPDHs Are Allowed to Work

Criteria Which Must be Met to Obtain an Expanded Practice Permit
This study surveyed current EPDHs, both practicing and non-practicing, with the purpose of assessing perceived barriers to practicing unsupervised and better educating students to begin EPP practice upon graduation. Specific research questions included:
If participants are currently practicing as an EPDH, what specific barriers do they face that make it challenging to practice in this role?
If participants are not currently practicing as an EPDH, what specific barriers have kept them from practicing in that role?
Do specific characteristics like level of education, years since graduation, or years holding an EPP increase the likelihood of utilizing the expanded practice permit?
How well does a specific institution which grants at least 500 hours of practice on patients in “limited access” settings prepare students to begin independent practice upon graduation based on reported barriers?
The results of this study will be used to advise students, further develop the dental hygiene curriculum at the authors' institution in support of independent practice and to suggest future directions for eliminating barriers to independent practice in Oregon as a whole to address the need for improved access to care.
Methods and Materials
In the fall of 2011, a list of all current EPDHs was obtained from the Oregon Board of Dentistry (n=186). A convenience sample of 2% was selected to pilot test the survey. Subsequent revisions were made according to feedback from the pilot testers. Following approval of the Pacific University Institutional Review Board with exempt status, the survey was mailed to all EPDHs in the state of Oregon in November 2011, with the exception of those included in the pilot test. Data were collected using a self-administered survey. A follow-up mailing was sent in December 2011 to all non-respondents. To maintain confidentiality, the surveys were numerically coded. The linkage file was maintained solely to facilitate the second mailing (a second survey was only sent to non-respondents). Once data collection was completed, the linkage file was destroyed. The mailing included a consent document explaining the purpose of the study and that it was confidential. In addition to a copy of the survey and the consent document, a business reply envelope was included (signed consent was not requested; consent was implied by return of the questionnaire).
The 16-item questionnaire contained both closed and open-ended questions that assessed the following areas: demographics, income from EPDH practice, amount of services provided, details of EPDH practice and perceived barriers to practicing as an EPDH. This article focuses on the demographics and perceived barriers sections. The amount of services provided and details of EPDH practice has been addressed in a separate report.14
When analyzing open-ended qualitative data related to barriers, 2 investigators determined preliminary categories to be able to do quantitative analysis of the data. Each investigator categorized the answers individually and the answers were then compared. Additional categories were added if at least 3 individuals answered similarly. If a response had less than 3 respondents reporting similarly the response was placed in the “other” category. Anywhere consensus could not be reached on a particular answer it was also placed in the “other” category. Ultimately, open-ended responses were categorized numerically for the purpose of statistical analysis.
The data were analyzed using SPSS (version 20, IBM). Frequency distributions are provided to describe the findings, and Chi-square tests using the Freeman-Halton extension of the Fisher exact test were used to investigate whether possible factors such as length of time holding EPP, level of education and years since graduation influenced the likelihood of EPDHs to be practicing in a setting which requires an EPP. For level of education, the sample contained 2 certificate holders; therefore, Certificate/Associates degrees were combined.
Results
The response rate for the survey of EPDHs was 39% (n=71). Approximately 41% (n=29) of the respondents were currently using their EPP and an additional 21% (n=15) were planning to start their own independent practice. The average age of the EPDH was 49, with a range of reported ages from 25 to 71 years of age. Sixty-two percent of the sample has held their EPP for 3 years or less (n=41). Of the current practicing EPDHs, the average weekly hours working unsupervised is 9.3 hours (n=25). On average, unsupervised practice comprises 22% of their total annual income (n=27). The highest level of education held by the sample was a bachelor's degree (58%, n=39). All demographic data is summarized in Table I.
Barriers faced by EPDHs were examined for both practicing and non-practicing EPDHs. The number of responses is larger than the sample size for each group because participants were allowed to report multiple barriers. For non-practicing EPDHs the most frequently perceived barriers were: currently working in another setting (21%, n=14), lack of business knowledge (15%, n=10), time (10%, n=7), inability to make a salary/living wage (10%, n=7) and start-up costs (10%, n=7) (Figure 3).
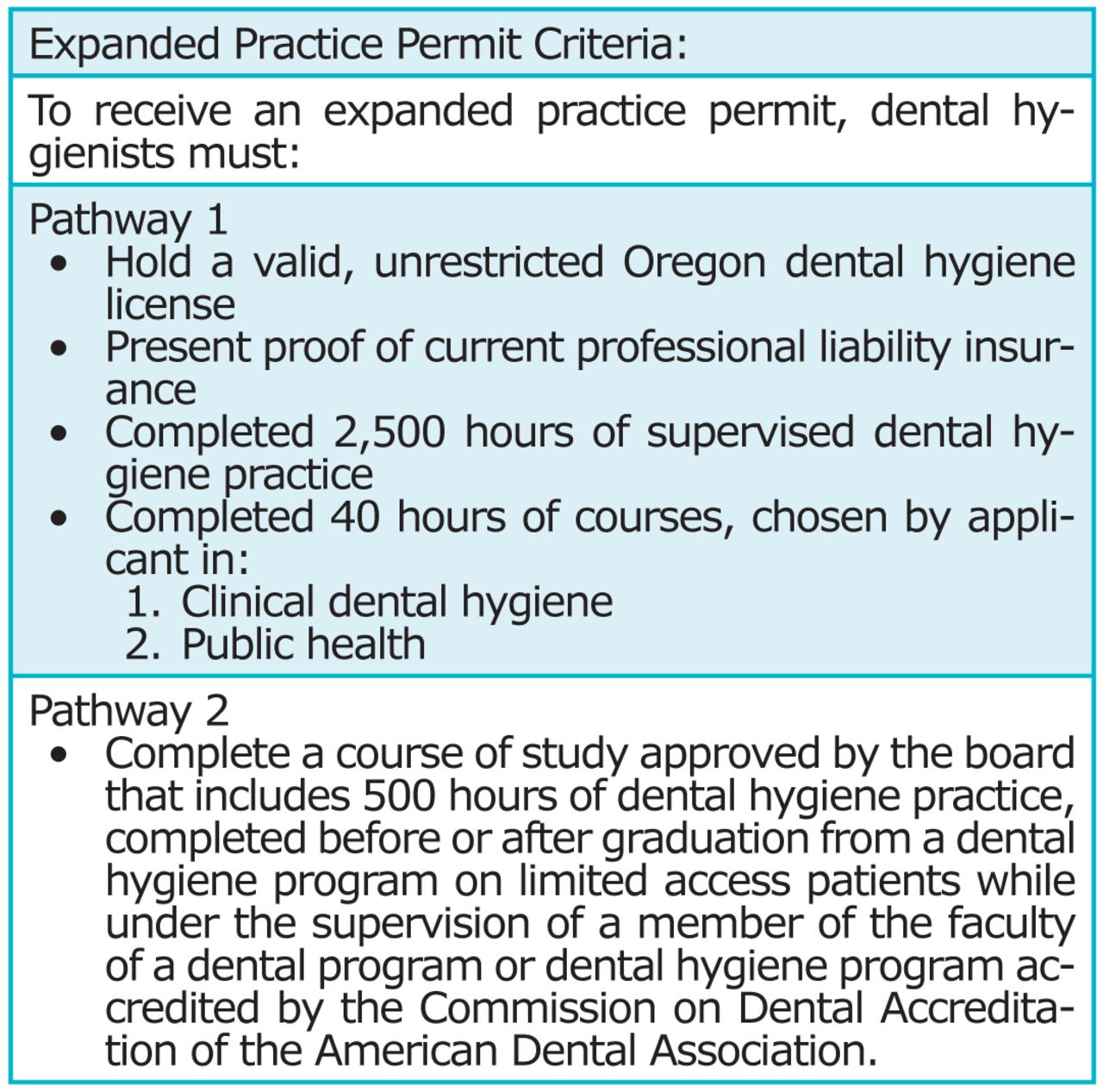
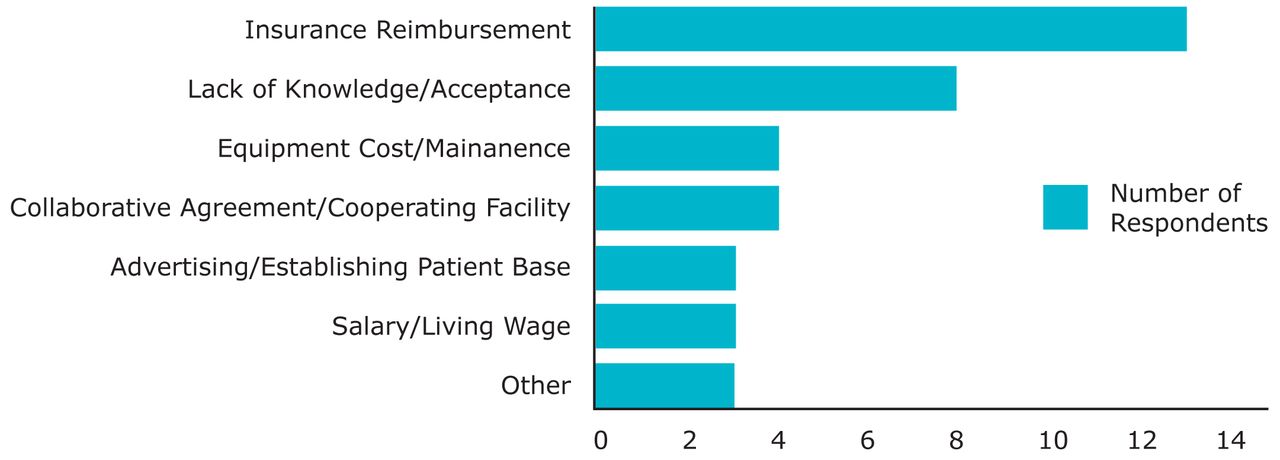
For practicing EPDHs, the most frequently cited barriers were: challenges with insurance reimbursement (39%, n=13), lack of knowledge/acceptance (21%, n=8), equipment cost/maintenance (11%, n=4), and lack of collaborative agreement/cooperating facility (11%, n=4) (Figure 4).
Chi-square tests using the Freeman-Halton extension of the Fisher exact test were used to explore possible relationships contributing to the likelihood of EPDHs to be practicing currently. While no statistically significant results were found, there were several trends identified in the sample of practicing EPDHs. The highest percentage of practicing EPDHs have held their EPP for 3 years or less at 21% (n=14) (Table II). The highest percentage of practicing EPDHs held a Bachelors degree or an Associates/Certificate at 19% (n=13) and 18% (n=12), respectively (Table III). The largest percent of practicing EPDHs had greater than 20 years since graduation, 20% (n=14) (Table IV).
Discussion
Although some form of the EPP has existed in Oregon since 1997, the largest percentage of the existing EPDHs have only had their permit for 3 years or less, which indicates an increasing support of Oregon dental hygienists for unsupervised practice. According to the Oregon dental board, the number of EPDHs in Oregon has increased from 186 to 356 since this survey was completed. This is a near double increase in the past 2 years. This increase is likely due to the abilility to obtain an EPP through the new pathway (pathway 2). While the majority have held their permit for 3 years or less, nearly half the sample of EPDHs are over 50 years old and have been out of dental hygiene school for longer than 20 years. This suggests that dental hygienists who have been practicing traditionally show strong interest in moving toward alternative settings to provide care. Authors attempted to evaluate whether concrete demographic characterisitics like level of education, number of years holding an EPP and years since graduation influnced the likelihood of EPP holders to be practicing. Unfortunately, a significant indicator of whether participants were more likely to be utilizing their EPP to provide care was not found in this study. Characteristics that influence the likelihood of EPP holders to be practicing are much more difficult to measure, although one previous study found that a motivation to attain independent decision making and a strong dedication to providing services to underserved populations influence the likelihood of individuals to practice using their EPP.13
Descriptive Statistics of Responding EPDHs
The data demonstrate that both practicing and non-practicing EPDHs perceive similar barriers to providing care to underserved populations. Both groups cited insurance reimbursement as a challenge, but a much higher percentage (61%) of practicing EPDHs reported reimbursment as an issue and nearly half stated they have never received insurance reimbursement. This is contrary to what was reported in the Dental Hygiene Professional Practice Index, which gave Oregon a rank of excellent in the area of reimbursment compared to other states with independent practice legislation.15 Non-practicing EPDHs reported reimbursment as a concern but much less so than practicing with only 4 individuals citing it as a barrier. This is most likely percieved as less of a challenge due to lack of experience in providing care in a limited access setting.

Perceived Barriers of Non-Practicing EPDHs (n=46)
*Total barriers exceeds number of participants because many participants reported more than one barrier.
It has been suggested that expanding the practice of dental hygienists could be a potentially significant income source.16 Yet both groups saw the inability to make a decent salary or living wage as a barrier. This study's findings suggest the majority of practicing EPDHs make less than $10,000 a year using their EPP. A larger percent of non-practicing EPDHs, 15% compared to 10% of practicing EPDHs, saw this as a barrier. This may indicate that motivation for those utilizing their EPP is not direclty linked to the income that it provides. Other motivating factors cited by Battrell et al included the desire to obtain independent decision making and a strong desire to serve underserved populations.13 These factors may outweigh the need for independent practice to supply a significant portion of income to those utilizing it.
Finally, both groups cited lack of knowledge as a barrier. Non-practicing EPDHs reported lack of knowledge regarding how to begin an independent practice, business knowledge and knowledge of the laws. Participants of the 2005 qualitative study of Oregon EPDHs identified a sense of entrepreneurship and marketing skills as keys to success.13 In addition, Astroth, et al report that the majority of independently practicing dental hygienists in Colorado had additional education in business management.17 For non-practicing EPDHs there is an apparent necessity of education associated with starting a business as well as a call for understanding the most current legislative advances in independent practice for dental hygienists in Oregon. Practicing EPDHs reported a different type of lack of knowledge which relates to acceptance and education on the part of dentists and the community. This included lack of knowledge for caregivers regarding the services provided by EPDHs, as well as lack of knowledge in the community as to what EPDHs can do. Removing this barrier would require additional education for the communities in which EPDHs serve.
Many barriers cited were unique to either practicing or non-practicing EPDHs. A barrier faced by practicing EPDHs was equipment cost and maintenance. In addition, establishing a patient base and advertising services were also cited as barriers. When minimal salary and ability to get reimbursed for services is low, unexpected costs of equipment and uncertainty of available patients to treat threaten EPDHs ability to continue providing care to underserved populations. As independent practice becomes more common, options to reduce barriers for EPDHs already practicing become extremely important.

Perceived Barriers of Practicing EPDHs (n=21)
*Total barriers exceeds number of participants because many participants reported more than one barrier.
Another barrier faced only by practicing EPDHs is securing a collaborative agreement with a dentist. A collaborative agreement allows an EPDH to administer local anesthetic and gives the EPDH additional prescriptive power. Lack of dentists' support for hygienists practicing independently has also been reported in other studies.16,18 One reason dentists may not support independently practicing dental hygienists is the perceived threat they may pose to patients seeking care from a dentist. However, having care provided by an independently practicing dental hygienist may not necessarily deter patients from seeking routine dental care. This item was specifically measured in a survey of patients treated by independently practicing dental hygienists in California. In that study, at the 24 month follow-up almost 90% of the patients had been seen by a dentist within 12 months of being treated by an independently practicing hygienist.19,20 It appears that, in California, patients who are treated by independently practicing dental hygienists are not less likely to seek routine care from a dentist as a result. In addition, EPDHs in Oregon are required by law to refer patients at least once per year to a dentist who is available to treat them. If patients treated in Oregon are similar to those treated in California, triage care with referral provided by the dental hygienist may increase the rate at which this population seeks care with a dentist. Further research is necessary to test this hypothesis.
The largest barrier seen by non-practicing EPDHs is that they are currently practicing somewhere else. These settings ranged from private practice to public health and education. While working in another setting might be viewed as more of a personal choice rather than a barrier, participants stated it was a barrier. Another barrier reported was a lack of opportunity which may more accurately represnt why working in another setting was cited. While holding an EPP shows strong support for dental hygienists practicing in unsupervised settings, additional barriers such as start up costs, too few internship settings and mentors, and lack of experience are preventing EPP holders from entering into unsupervised practice. When EPDHs spend the majority of their time practicing elsewhere there is little time to pursue the elimination of other barriers. With a growing number of EPDHs in the state of Oregon, there is a responsibility to give individuals the tools necessary to begin practicing independently so that this practice model does in fact reduce the access to care issue.
Non-practicing EPDHs had a variety of barriers that keep them from utilizing their EPP. Reasons varied widely which is why the “other” category received the second most responses. Since 3 or more respondents who cited a particular barrier were required to become a category, many responses were placed in the “other” category. Some examples included: “I'm holding an EPP in support for advancement of the profession but have no personal interest in using it,” “I just haven't branched out yet, although I live in an underserved area,” “I'm late in my career” and “I am not currently practicing.”
Implications for Education
The addition of pathway 2 to the Practice Act has made it easier for new graduates to obtain an EPP. Targeting the population of new dental hygiene graduates who have not already obtained employment could potentially increase the number of hygienists practicing independently since already working in another setting was the greatest barrier for non-practicing EPDHs. Many of the documented barriers found through this study for both practicing and non-practicing EPDHs could be reduced through additional curriculum focused on practicing independently. With 35 states allowing direct access, the question of educating new dental hygienists to pursue this career path must be addressed. Argument could be made that educators have the responsibility to prepare students for the additional professional aspects of direct access in the states that allow it.
Percent of Practicing EPDHs Based on Length of Time Holding EPP (n=66)
Percent of Practicing EPDHs Based on Degree Type (n=67)
Percent of Practicing EPDHs Based on Years Since Graduation (n=70)
Currently, the Commission on Dental Accreditation (CODA) standards do not explicitly require dental hygiene programs to educate students on aspects relating to independent practice. However, CODA does require graduates to be competent in assessing, planning, implementing and evaluating community based oral health programs including health promotion and disease prevention activities, and the curriculum must include content in community dental/oral health.21 CODA concepts that relate to independent practice are the ability to competently plan and implement community based oral health programs with the intention that students will be able to apply community dental health principles to prevent disease and promote health. With dental hygiene curriculums already being tightly constructed, it is difficult to entertain the idea of adding additional material. Authors believe that courses being taught to fulfill these CODA requirements could slowly begin to incorporate independent practice as a topic. This is a good starting point and may already exist in many schools, but does not address all of the barriers perceived to entering independent practice.
At one educational institution in Oregon, Pacific University, curricular changes have been implemented to reduce the barriers for students graduating with the intention of practicing indpendently with limited access populations. Specific curricular changes address the barriers of lack of experience, business knowledge, and reimbursement. These include an expanded practice rotation, implemented in 2011, where students provide dental hygiene services in limited access settings to gain experience with this patient population. For this rotation, students work alongside an EPDH to see firsthand what goes into practicing indpendently. In addition, students take an indpendent practice course in the summer of their senior year, also implimented in 2011. This course gives an overview of independent practice for dental hygienists including state regulation, employment opportunities, business models, marketing, reimbursement and community relations.
Business knowledge is also a key piece to having a successful independent practice and lack of business knowledge was reported as a barrier by non-practicing EPDHs. Since 2007, students at Pacific University have taken a business management course where they learn basic principles of business with emphasis on application of business management skills in dental health care settings.
Cultural competence has also been reported as an important skill for expanded practice dental hygienists in Oregon due to a large number of Hispanic populations being seen by EPDHs.13 While this was not an aspect directly measured in this study, it is an additional way Pacific University prepares students to work with limited access patients. Since the program's inception, students have been required to take 2 semesters of Spanish for dental professionals and treat primarily Spanish speaking patients in the school's clinic as well as many of their off campus rotations.
Although Pacific graduates comprised only 9% of the EPDHs in the current survey, at the time Pacific had only graduated 4 cohorts of students. According to the Oregon dental board, since this study was completed the percent of Pacific University graduates holding an EPP has grown from 9 to 27% of the total EPP holders in Oregon. While the percentage of EPP holders who graduated from Pacific has grown significantly since many curricular changes were implemented, whether these changes have influenced their likelihood to practice in a setting which requires an EPP is yet to be measured. It is apparent, at least at one school in Oregon, that the addition of pathway 2 has been a successful way to increase the number of EPP-holders in the state.
Unfortunately, not all the barriers discovered through this study can be addressed in education. There are still many practicing and non-practicing EPDHs who have completed their education and need support to enter independent practice in Oregon. The current sample is also primarily older and more experienced. Potential avenues to addressing these barriers are: business focused continuing education courses for individuals holding an EPP and mentorship programs with currently practicing EPDHs. Other avenues could include enlisting the help of community leaders, community clinics, Head Start programs and long term care facilities. The solution will no doubt need to be a multi-faceted endeavor.
Study Limitations
There were several limitations to this study, with one of the most significant being the sample size. Because this survey was also an outcomes assessment asking EPDHs to report the amount of services provided and details of EPDH practice, EPP holders who are not currently practicing may not have thought the survey was applicable to them. The questions about perceived barriers were at the end of the survey. This limitation had an impact on the ability to conduct statistical analysis because there were not enough practicing and non-practicing EPDHs in each of the categories to be able to find any statistical significance. An additional limitation was anticipating how modest a salary EPDHs received with $10,000 or less being the only possible option, which many EPDHs reported making much less than $10,000 annually. If this had been an open-ended question, it would have better allowed for reporting smaller income ranges. When asked about reimbursement, a large number of practicing EPDHs reported never receiving any reimbursement but several individuals wrote in that they had never tried. This would have been a valuable option that was not included. Finally, the authors were not able to establish survey performance reliability. The survey has been administered only 1 time, so test-retest reliability could not be determined. In order to keep the survey to a minimal length, no redundant questions were included to evaluate internal reliability. To facilitate data entry and consistency of information, every survey mailed was identical, so no alternate-form reliability was established.
Recommendations for future research include exploring how curricular changes have influenced Pacific University graduates' likelihood to enter into independent practice settings. Whereas the business management and Spanish course have existed since the beginning of the program in 2006, the expanded practice rotation and independent practice course have only been taught since the fall of 2011 when this survey was conducted. In addition, investigating how dental hygiene programs in other states with some type of independent practice prepare their students to pursue this avenue of providing care is important. Opinions as to whether dental hygiene programs should have the task of preparing dental hygienists to practice unsupervised in direct access states or if it should be done through other pathways should also be examined.
Conclusion
Data from this study indicate that there are an increasing number of new EPP holders in Oregon, but less than half are actually providing care as an EPDH to underserved populations. Lack of business knowledge, lack of experience, insurance reimbursement, start-up costs and the inability to make a living wage are barriers non-practicing EPDHs face when deciding whether or not to utilize their EPP. If these barriers can be addressed during dental hygiene education, the potential exists to increase the number and impact of EPDHs in Oregon. For dental hygienists who have already completed their education without the benefit of new curriculum, addressing independent practice, continuing education courses in business management and independent practice strategies, and paid internships with experienced expanded practice dental hygienists may also be helpful in facilitating the transition to independent practice and to facilitate increased access to care.
Footnotes
-
Amy E. Coplen, RDH, EPDH, MS, is an Assistant Professor, School of Dental Health Science, Pacific University. Kathryn P Bell, RDH, MS, is an Assistant Professor, School of Dental Health Science, Pacific University.
-
This study supports the NDHRA priority area, Health Services Research: Investigate how alternative models of dental hygiene care delivery can reduce health care inequities.
- Copyright © 2015 The American Dental Hygienists’ Association





{kind=link}
{kind=link}
{kind=link}
{kind=link}