



Abstract
Purpose: The purpose of this study was to identify the cultural climate of southwestern dental colleges, from the perspective of dental hygiene and dental students.
Methods: The Cultural Attitudes and Climate Questionnaire was used to measure cultural climate. It contained 57 items related to campus experiences, cultural comfort, diversity awareness, racial pressures, fair treatment, respect, lack of support, patient care and overall satisfaction. The survey was administered to 508 dental and dental hygiene students at 5 dental colleges.
Results: The response rate was 41% (n=239/508). Students reported not experiencing racial conflict or pressures (71 to 90%), being treated fairly and with respect (86 to 90%) and being comfortable interacting with and treating other cultures (70 to 91%). They also practiced culturally appropriate behaviors (54 to 92%). Those reporting diversity training (77.8%) were more likely to engage in 3 of the 6 awareness practices (p<0.033). Although all groups agreed their educational experience was rewarding (89.5%), African-Americans reported a significantly lower level of agreement than Whites (p=0.003) and Asians (p=0.008). Among all groups, satisfaction with their educational experience was significantly correlated with fair treatment (rho=0.441 to 0.511, p<0.001) and respect for other cultures (rho=0.391 to 0.441, p<0.001).
Conclusion: The students generally reported a positive cultural climate. Improvements could be made by focusing on fair treatment, respect for cultures and the African-American experience. Cultural competence training could be key to improving cultural climate, as positive outcomes from training were identified.
Introduction
Minority populations are increasing in the U.S.1 Clear evidence exists that there are disparities in health care among these diverse populations within the U.S.2 Minorities need and demand culturally appropriate health care services.3 Culturally competent care is critical for gaining patient trust, and health care providers must practice effective communication skills to engage patients of all cultural backgrounds for the delivery of appropriate care.4 To better serve these populations, health profession schools are being asked to diversify their student bodies, personnel and climate by such organizations as the Institute of Medicine and the Commission on Dental Accreditation.2,5
Why is Cultural Climate Important?
Cultural climate is defined as the culture of the institution in terms of how open and accepting it is of diverse groups of people, ideas, opinions and beliefs (Table I).6-9 Why is cultural climate important in an educational institution? First of all, ethnic diversity in higher education settings is associated with better educational experiences for all students.10 Also, cultural competence cannot be achieved in a homogeneous environment but requires the “in-depth exchange of ideas and beliefs across gender, racial, ethnic, cultural and socioeconomic lines.”5 Conversely, continual exposure to a hostile climate can negatively impact a student's academic achievement and psychological health.11
Increasing student diversity creates a richer multicultural environment which can improve learning.12 Chang and Le did a study in 2010 with Asian-American and Hispanic youths and found that perceived school multiculturalism had a significantly positive relationship (p<0.05) with ethno-cultural empathy and academic achievement. Thus, the way students perceived the diversity climate at their school increased their empathy for diverse individuals and improved academic achievement.13 In 2010, Simmons et al surveyed college students regarding the campus cultural climate and their acceptance of ethnic and racial diversity.14 The results were that appreciating positive interactions with other ethnic groups increased their acceptance of diversity, emphasizing the importance of interactions with different groups.
A cultural climate that supports diversity also facilitates achievement of cultural competence. In 2004, Novak et al measured dental students' perspectives on the importance of diversity and diversity training at seven different U.S. schools.1 They found that exposure to diversity and perceptions of competence to serve diverse patient populations were positively correlated. The students stressed that it was important to have a diverse composition of students, faculty and patient population, and a curriculum that prepared them to work with diverse ethnic and racial backgrounds. Similarly, Whitla et al10 and Hung et al15 found that medical students believed diversity and cultural competence were important to their development as clinicians.
What is the Current Cultural Climate?
The current cultural climate at health professional programs has not been thoroughly explored. In 2007, Hung et al surveyed medical students at one school to determine the racial/ethnic diversity and cultural competence of the campus.15 While most of the URM students felt that the school had succeeded in creating an encouraging cultural climate, a small portion did not feel that the university truly valued diversity. Most students felt that the lack of diversity at their school impaired the retention and recruitment of minority students.
Two studies in dental hygiene programs have shown a deficiency in cultural climates. They used the Cross-Cultural Adaptability Inventory that measures cross-cultural skills in four dimensions: emotional resilience, flexibility/openness, perpetual acuity and personal autonomy. In 2004, Magee et al used the Cross-Cultural Adaptability Inventory in 8 dental hygiene programs (n=188). The overall score of the dental hygiene students was lower than the Cross-Cultural Adaptability Inventory norm group, suggesting the need for cultural competence training.16 In 2009, DeWald and Solomon used the Cross-Cultural Adaptability Inventory to track dental hygiene cross-cultural skills over the course of the program, at initial orientation, at the end of the first year and the end of the second year (n=30).17 No significant improvement was identified in cross-cultural effectiveness over the course of the 2 year curriculum.
Definitions
Several studies suggest that cultural competence education at dental schools could be improved. In 2006, Saleh et al assessed the extent of cross-cultural education in U.S. dental schools.18 Only 29 of the 54 schools reported having formal training in their curriculum. They also found a lack of understanding about how to best incorporate cross-cultural education into the curriculum. Hewlett et al conducted a study in 2007 with fourth-year dental students to determine if the time spent on cultural training was sufficient to achieve competence in caring for patients of diverse cultural/racial backgrounds.19 Twenty-five percent reported that the time spent was inadequate. Female, URM, Asian/Pacific-Islander or unmarried students were more likely to report that the time was insufficient. In 2008, Wagner and Redford-Badwal surveyed dental students regarding their knowledge of cultures and using culturally appropriate practices in oral health care.20 They found that students believed using culturally appropriate practices was important, but they had insufficient knowledge about the groups they would treat in practice.
In general, minority college students report a less positive cultural climate. In 2000, Ancis et al assessed African-American, Asian-American, Latino/Latina and White students at a large, mid-Atlantic university.11 African-American students reported significantly more experiences with racial conflict and unequal treatment by faculty and staff. They also experienced more racial separation compared to Asian-American and White students. Both African-American and Asian-American students reported significantly more racism from faculty than White students.
Minority medical students have similar experiences. In 2004, Dyrbye et al surveyed 3 medical schools in Minnesota to examine possible differences in quality of life between minority and non-minority students.21 Minority students reported a lower sense of accomplishment, and experienced bias, discrimination, stereotyping, isolation, depression and burnout. They specifically reported more major illnesses, trouble finding child-care and isolation from their family support systems. In 2007, Odom et al identified lack of financial and social support, hardships with standardized testing, and ethnic/racial discrimination as barriers for minority medical students. Conversely, they identified strong support, professional exposure and financial assistance as mediators for their personal and academic success.22
Limited research has been done on the cultural climate in dental schools. Thus, the purpose of this study was to identify the cultural climate of southwestern dental colleges, for both dental and dental hygiene students, and what factors affect this climate. The specific research questions of this study were:
What is the cultural climate in southwestern dental schools, including diversity training?
Are there differences among racial/ethnic groups about the cultural climate?
Are some cultural climate factors associated with satisfaction with the dental school experience?
Methods and Materials
Population and Sample
The target population of this study was all fourth-year dental students and senior dental hygiene students attending dental colleges in the Southwest U.S. The study focused on these students because they were close to graduation and had the most experience with their school environments. Once invited, 5 of the 6 dental schools in the region elected to participate in the study. Each of these schools had both a dental and dental hygiene program, which allowed the identification of the cultural climate from both perspectives. The total population surveyed consisted of 181 senior dental hygiene students and 402 fourth-year dental students. Of this population, 239 completed the voluntary survey, yielding a response rate of 41%.
Instrument and Administration
This study used a modification of the Cultural Attitudes and Climate Questionnaire developed and validated by Helm, Sedlacek and Prieto.23 In 1998, they surveyed 566 students at a large, east coast university with this instrument. Factor analysis identified 11 scales with high alpha levels ranging from 0.55 to 0.70, with an overall reliability of 0.81.
This study used the following 11 scales:
Demographics
Campus experiences
Cultural comfort
Diversity awareness
Racial pressures
Fair treatment
Respect for other cultures
Lack of support
Patient care
Overall satisfaction
Cause of unfair treatment
The alpha levels for each of 11 scales ranged from α=0.732 to 0.968, with an overall mean of 0.870, indicating a high level of reliability. Using a 5-point Likert-type response, respondents reported their level of agreement with 56 statements. The last question was open-ended and allowed participants to add any additional information related to cultural climate.
A committee of 3 experts in survey design, data analysis and cultural diversity reviewed the survey instrument. After approval by the institutional review board at Texas A&M Health Science Center Baylor College of Dentistry (expedited IRB 2012-31), the survey was pilot tested. No changes were made to the survey instrument, because the pilot study verified ease and clarity of the questionnaire. The survey and consent protocol were distributed by administrators at each school. Completion and return of the survey constituted informed consent.
Demographics of Participants
Data Analysis
Following data collection, results were coded and entered into SPSS software program for statistical analyses. Descriptive statistics, including frequencies and cross tabulations, were used to identify the cultural climate of the schools. Kruskal-Wallis and Mann Whitney U tests were used to determine differences between groups about the cultural climate. Spearman's correlation was used to examine associations between aspects of cultural climate and overall satisfaction. In order to protect against Type I errors when running a large battery of tests, the alpha level was set at α=0.001 rather than α=0.05. Cronbach's alpha tests were used to measure the reliability of the survey sections. Open-ended comments were transcribed and analyzed qualitatively for emergent themes.
Results
Demographics
Table II illustrates the demographics of the study participants. Of the 239 respondents, 60% were senior dental hygiene students and 40% were fourth-year dental students. The majority were White (64%), followed by Hispanic (15%), Asian or Pacific Islander (13%), Black or African American (6%), and Native American (2%). These categories represent the collapsing of 11 unambiguous categories based on ancestry. The majority were female (77%) and grew up in the U.S. (90%). The age range was 21 to 56 years of age, with a mean of 27.2 years and a standard deviation of 5.2 years.
The racial/ethnic make-up of the dental respondents mirrored that of the 5 southwestern U.S. schools from which they were drawn and were not significantly different than the dental hygiene respondents (X2=2.969, p=0.709).24 Overall, they were 37 and 36% non-White, respectively. The White group was slightly over-represented in the sample and the Asian group is somewhat under-represented. The 3 URM groups were remarkably well represented. None of these small differences were significant (X2=2.056, p=0.725).
Campus Experiences
Cross and Intra-Cultural Comfort
Cultural Climate
For Tables III, IV, V, VI, VII and VIII, the 5-point Likert-type scale was collapsed into a 3-point scale. As illustrated in Table III, a preponderance of students felt racial conflict/tension was rarely present on their campus. Students responded “never” or “seldom” to interracial tensions in the classroom (90%), racial conflict on campus (89%), and racial and ethnic separation (76%). Most students were also not resentful of others whose race and ethnicity were different from their own (84%).
As seen in Table IV, students reported being quite comfortable with cross and intra-cultural situations. They reported being the most comfortable with people whose racial background was different/ the same as their own (85 and 89%), and going to see a faculty member of their own race (85%). They reported being the least comfortable saying what they thought about racial and ethnic issues (68%), and when they were the only person of their racial or ethnic group (70%).
As seen in Table V, the majority of students did not report experiencing racial pressures. Only 10% of the students agreed that they needed to minimize various characteristics of their racial/ethnic culture (such as language and dress) to be able to fit in at their dental school and were pressured to participate in ethnic activities. Slightly over one-fourth (27%) did agree that there were expectations about their academic performance because of race or ethnicity.
The majority of the students believed they were treated fairly. Students reported fair treatment (“fairly” or “very fairly)” from classroom faculty (90%, n=216), clinical faculty (86%, n=206) and other students (86%, n=206). Over 84% of students reported that race/ethnicity, gender, age, sexual orientation and religion were not (“never” or “seldom”) the cause of unfair or insensitive treatment at their school.
Racial Pressures
Lack of Support
Students felt there was a high level of respect shown for other cultures. Respect by faculty for students of different racial and ethnic groups was reported by 91% of students (n=215). Students reported “often” or “almost always” for the occurrence of friendship between students of different racial and ethnic groups (87%, n=207) and respect by students for other students of different ethnic groups (87%, n=206).
As seen in Table VI, the majority of students did not report much difficulty in getting support from faculty or students. Students reported not (“never” or “seldom”) having difficulty receiving help or support from classroom faculty (64%), clinical faculty (62%) or other students (62%). On the other hand, about 30% did report difficulty getting support from the 3 groups.
Students indicated they were comfortable treating patients the same as their own race/ethnicity, gender, religion, sexual orientation and age (90 to 92%, n=213 to 220) and different from their own (88 to 91%, n=206 to 214). Generally, treating patients “different from my own” received lower scores than “same as my own,” but these differences were not statistically significant.
Thirty-nine students provided comments regarding cultural competence and/or the diversity climate at their dental school. The 3 most common themes were:
No discrimination exists at their institution (n=13)
Discrimination against minority students does exist (n=6)
Preferential treatment exists for minority students (n=5)
As the largest number of comments was about discrimination not being present at their school, this supports the quantitative results of this study.
Diversity Awareness and Training
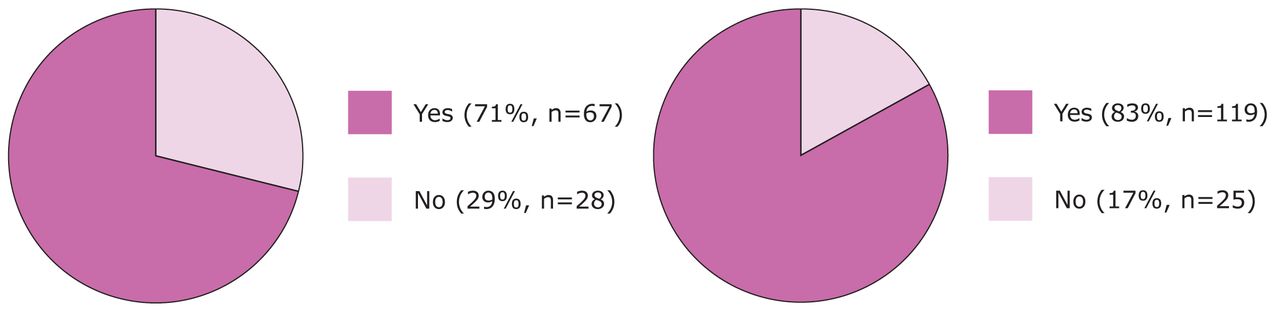
The frequency of diversity training at dental schools, shown in Figure 1, was 83% for dental hygiene students, 71% for dental students and 78% overall. As shown in Table VII, students “agreed” or “strongly agreed” that they understood racial/ethnic differences (92%) and had stopped using language that might be offensive to others (83%). The lowest majority at 54% “agreed” that they handled negative language used by another in such a way as to try to educate the other person.
Diversity Awareness
Overall Satisfaction
In general, students believed that they were culturally aware in their thinking and behavior, but that their dental school experience did not contribute to this (<50% agreed). However, Mann Whitney U tests indicated that the trained students were more likely to agree that they engaged in the following behaviors: discussing topics related to cultural awareness with friends (p=0.020), stopping themselves from using language that might be offensive to others (p=0.002) and handling negative language used by another in such a way to try to educate the other person (p=0.032).
Overall Satisfaction with Cultural Climate
Table VIII illustrates that students generally “agreed” that their college climate was positive. They agreed (“agreed” or “strongly agreed”) that their educational experience was rewarding (90%), they felt a sense of belonging in their school (89%) and the school provided an environment for free and open expression of ideas, opinions and beliefs (79%).
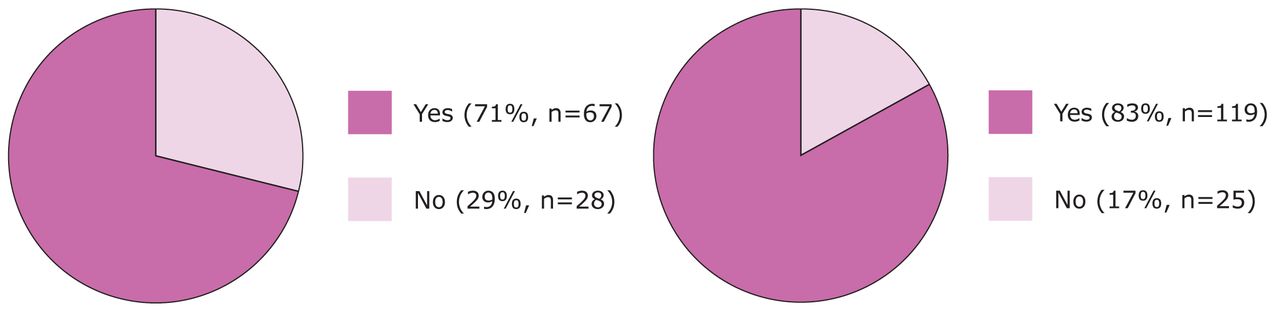
A: Frequency of Diversity Training Among Dental Students
B: Frequency of Diversity Training Among Dental Hygiene Students
Total percent of training among both groups – Yes: 78%, No: 22%
Differences among Groups about Cultural Climate
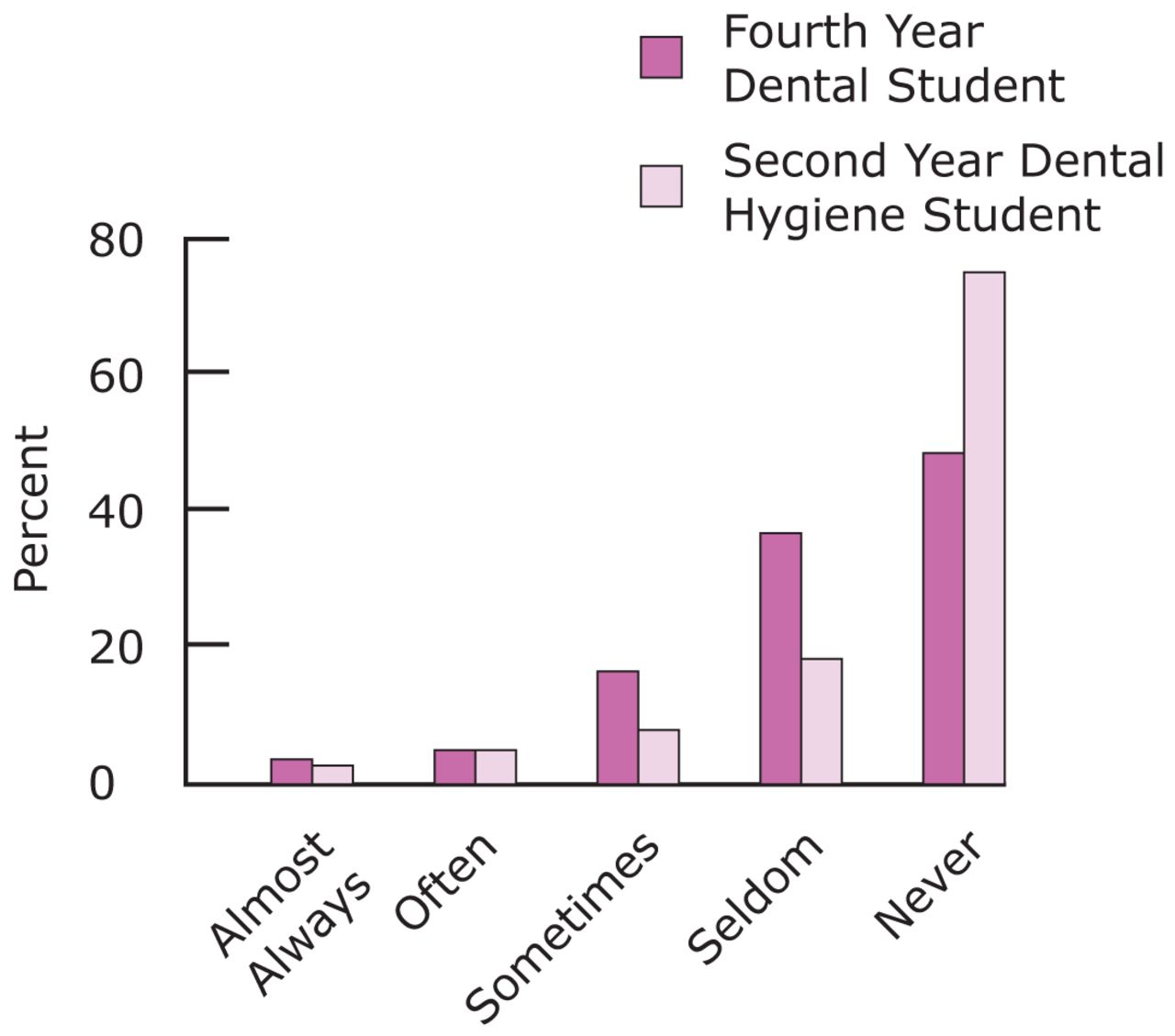
The Mann Whitney U test indicated a significant difference (p<0.001) between the dental and dental hygiene students regarding the extent of racial conflict on campus. As illustrated in Figure 2, dental hygiene students reported significantly less racial conflict on campus (76% “never”) than dental students (50% “never”). Among all the students, there was no significant gender difference regarding perceptions of racial conflict (Mann Whitney U test, p=0.582).
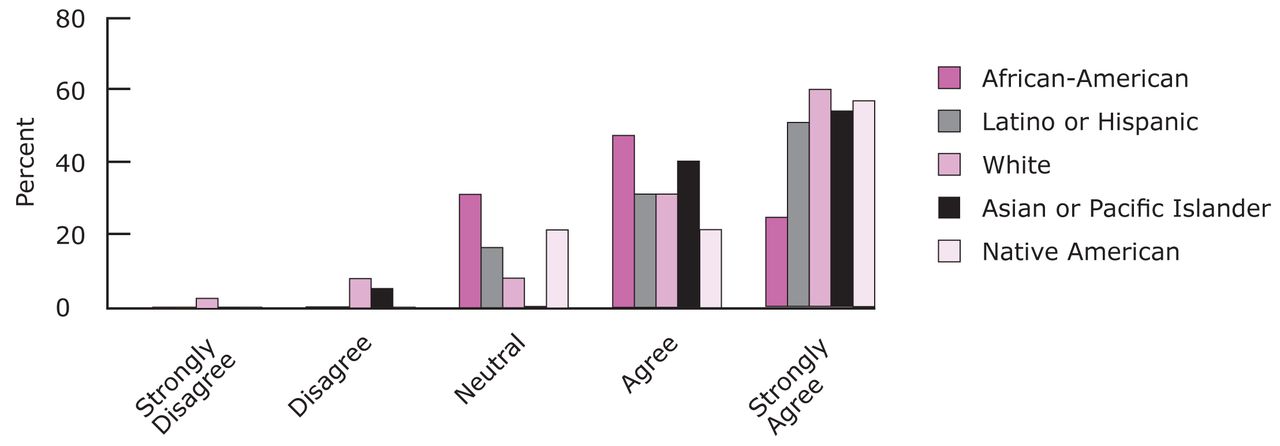
African-American students reported somewhat less positive experiences than the other student groups. As seen in Figure 3, a Kruskal-Wallis test indicated a significant difference among the ethnic groups regarding their agreement as to whether their educational experience was rewarding (p=0.047). Mann-Whitney U tests showed that African-Americans reported a significantly lower level of agreement than Whites (p=0.003) and Asian-Americans (p=0.008). The other between group differences did not approach significance (p>0.30), except for African-Americans reporting marginally less agreement than Hispanics (p=0.062). Also, compared to Whites and Asian-Americans, African-American students reported having significantly greater difficulty getting help from clinical and classroom faculty and other students (p≤0.024).

Racial Conflict According to Program
Dental hygiene students reported significantly less racial conflict than dental students (p<0.001).
Factors Influencing Satisfaction with Cultural Climate
Spearman's correlations indicated that overall satisfaction with the educational experience was significantly correlated with fair treatment by classroom faculty (rho=0.487, p<0.001), clinical faculty (rho=0.511, p<0.001) and other students (rho=0.441, p<0.001). Significant correlations with overall satisfaction were also found with respect for other cultures; specifically, respect by faculty for students of different ethnic groups (rho=0.391, p<0.001), respect by students for other students of different ethnic groups (rho=0.441, p<0.001) and friendship between students of different ethnic groups (rho=0.422, p<0.001).
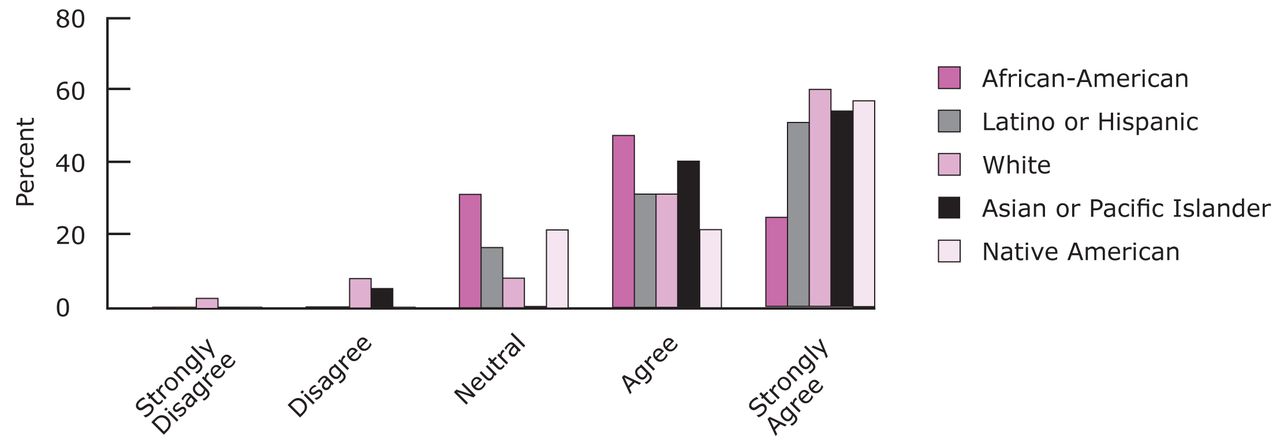
Overall Satisfaction According to Race/Ethnicity
For the question “overall my educational experience here has been a rewarding one,” responses for African-American students differed significantly from those of Whites and Asian-Americans (p≤0.008). Differences between pairs of other ethnic groups were not significant (p>0.05).
Discussion
Cultural Climate
In this study, the dental and dental hygiene students generally reported a positive cultural climate at their southwestern dental schools. They rarely experienced racial tension or pressures, were treated fairly and with respect, got the support they needed and were comfortable interacting with people of different race/ethnicity and culture. The students also reported that their schools provided them with free expression of their ideas and beliefs and that they “belonged” at their school. Overall, their educational experience was rewarding to them. The overwhelming majority did not believe that race/ethnicity caused unfair treatment. These researchers had anticipated other factors might cause unfair practices. However, none of the factors evaluated – religion, sexual orientation, age or gender – were perceived as causing insensitive or unfair treatment to any great degree.
Diversity Training
In terms of diversity awareness, students highly agreed they practiced the behaviors of culturally competent individuals. Although almost 80% of the students reported having diversity training at their present school, they did not believe their school experiences contributed to their diversity awareness behaviors. However, this study showed that their training probably did influence their behaviors, such as stopping themselves from using offensive language and using negative language as an opportunity to educate people about cultural awareness. Diversity training does seem to be making a positive impact on the cultural climate of southwestern dental schools.
Differences Among Groups about Cultural Climate
There were some differences in how the cultural climate was perceived by various groups. African-Americans reported a significantly less rewarding experience than Whites and Asians and had more difficulty getting help. Other studies have reported that African-American students have a less positive experience than other groups on campus.11,25,26 This may be a phenomenon of our broader society rather than just dental schools, but it still needs to be addressed. Also, dental hygiene students experienced less racial conflict than dental students. This cannot be explained by the proportion of minority students in the 2 programs, because these were similar. It also cannot be explained by gender differences, because, across programs, there were no significant differences between males and females regarding the perception of racial conflict. Therefore, this must be due to program differences rather than gender. Possibly some strategy or positive behaviors are in the place in dental hygiene programs that need to be identified and introduced into dentistry.
A small number of students believed preferential treatment was given to minorities at their college, favoring them over White students. The view was expressed that the increasing diversity of the classes and the focus on cultural competence was giving minority students an unfair advantage. Hopefully, these attitudes will change with training and the passage of time.
Factors Influencing Satisfaction with Cultural Climate
These researchers sought to identify cultural climate factors that positively influenced satisfaction with the dental school experience. This information could help schools focus their efforts on improving their cultural climates. The highest significant correlation in this study was between fair treatment from faculty and students and having a rewarding educational experience. Significant associations were also found between respect for other cultures by faculty and students and a rewarding educational experience. Helm, Sedlacek and Prieto, developers of the Cultural Attitudes and Climate Questionnaire, also found overall satisfaction was significantly correlated with respect for other cultures and that fair treatment by students and faculty members had the highest correlation with overall satisfaction among all racial/ethnic groups.23 Fair treatment and respect for all cultures should be a focus of cultural competence training.
Recommendations
The research findings indicate that these southwestern dental colleges are doing well at providing a positive environment for their students. However, maintaining or improving the cultural climate is an ongoing process. Formally assessing cultural climate with an instrument like the Cultural Attitudes and Climate Questionnaire could assist these and other colleges in achieving a highly inclusive environment.23 Dental schools also need to continue diversity/cultural competency training for their students, as well as for faculty and staff, since diversity training was associated with the increased practice of some culturally appropriate behaviors. Other studies of dental students have also shown improvement in knowledge and self-awareness following cultural competence training.17,27 These results stress the importance of training and the need to assess its impact on student behavior. Schools should investigate the best ways to incorporate diversity/cultural competence training into their curricula and share best practices with each other.
We can suggest a few promising approaches for cultural competence training. Since cultural competence is primarily about communication, a method called “nonviolent” or “collaborative” communication is suggested. Though not well researched in this context, this conflict resolution method is based on the premise that all people have the capacity for compassion and only resort to harmful behavior when they do not have more effective strategies for meeting needs. The training teaches how to identify and express one's needs, hear the same from others and develop strategies for meeting needs across cultures.28 Also, the U.S. Office of Minority Health is developing an online training course for oral health professionals for release in 2014.29 Beyond assessing knowledge, students should be assessed for behavior changes, such as their confidence in providing care for a diverse population and working in a diverse health care team, and their willingness to treat URM, poor and underserved populations after graduation.
Future research could assess cultural climate in other parts of the U.S. as this study only examined southwestern dental colleges. It could also address how to improve the experience of African-American students in dental colleges. The best approaches for faculty, students and staff achieving cultural competence through diversity/cultural competence training should also be further explored.
Conclusion
Regarding the research questions, southwestern dental schools appeared to be doing well at providing a positive cultural experience for their students, especially the dental hygiene programs. There was not any obvious racial conflict or strife. Diversity/cultural competence training did increase the practice of culturally appropriate behaviors and is probably key to improving cultural climate. African-American students generally viewed the cultural climate as less positive than other ethnic/racial groups and fair treatment, respect for other cultures and comfort in cross-cultural interactions were associated with satisfaction with the dental school experience.
Ultimately, creating a positive cultural climate for dental and dental hygiene students will increase the willingness and competence of the graduates to treat a diverse population and so increase access to dental care in this country. These practitioners will also touch thousands of lives over the course of their careers and teach tolerance by example. In a world where bigotry and associated behaviors, such as bullying and hate crimes, have not diminished and seem to be intensifying, there is a great need for culturally competent oral health care practitioners who contribute to a more tolerant and healthier world.
Footnotes
-
Mary T. Vu, RDH, MS, is a Clinical Assistant Professor, Caruth School of Dental Hygiene. Ann L. McCann, RDH, PhD, is a Professor and Director of Planning and Assessment, Academic Affairs. Emet D. Schneiderman, PhD, is a Professor, Department of Biomedical Sciences. Janice P. DeWald, DDS, MS, is a Professor, Director and Chair of Dental Hygiene, Caruth School of Dental Hygiene. Patricia R. Campbell, RDH, MS, is a Professor, Graduate Program Director, Caruth School of Dental Hygiene. Barbara H. Miller, DDS, MS, is an Associate Professor and Executive Director, Recruitment and Admissions. All authors are at Texas A&M University Baylor College of Dentistry.
-
This study supports the NDHRA priority area, Health Promotion/Disease Prevention: Investigate how diversity among populations impacts the promotion of oral health and preventive behaviors.
- Copyright © 2015 The American Dental Hygienists’ Association





{kind=link}
{kind=link}
{kind=link}