



Abstract
Dental hygienists (DHs) are well positioned to be part of primary care teams to increase access to oral health care, particularly for those who encounter barriers to oral care, such as pregnant people. The Michigan Initiative for Maternal and Infant Oral Health (MIMIOH) integrates DHs into obstetrics and gynecology (OB/GYN) clinics in federally qualified health centers (FQHCs) to improve pregnant people’s oral health. Evaluation of the MIMIOH program revealed that selecting DHs with personal characteristics desirable for integrated-care delivery was a major factor for successfully integrating DHs into OB/GYN clinics. Additionally, designing appropriate clinical workflows, gaining buy-in from prenatal health care professionals, presenting oral health care as part of prenatal care, having co-located OB/GYN and dental clinics, and maintaining adequate funding were all critical to program success. Analysis of Medicaid data showed that the MIMIOH model increased the percentage of pregnant people receiving oral health care at FQHC dental clinics. Innovative programs like MIMIOH add to the evidence that integrating DHs into primary care settings can increase access to oral health care, especially for those who face difficulties accessing the traditional oral health care system. There is great potential for DHs to leverage collaborative practice agreements and remote supervision to increase access to oral health care for the public. Providing DHs with autonomy to practice to the highest level of their scope of practice and permitting direct Medicaid reimbursement for DHs would make oral health care more accessible for underserved populations.
- dental hygienists
- federally qualified health centers
- medical dental integration
- prenatal health care
- oral health care
- public health
INTRODUCTION
In 2000, Oral Health in America: A Report of the Surgeon General emphasized that oral health is integral to overall health and should not be viewed separate from overall health.1 Since then, several federal reports have highlighted integrating oral health care and primary care as a promising strategy to expand access to oral health care and reduce health inequities; improve care coordination, health outcomes, and patient satisfaction; and reduce health care costs.2,3,4 A subsequent report in 2021, Oral Health in America: Advances and Challenges underscored the importance of integrating oral health care and primary care as a strategy to increase access to care for those who are underserved and to improve patient-care delivery and outcomes while reducing costs.5
Dental hygienists (DHs) are preventive oral health specialists and well positioned to be part of primary care teams that address oral and systemic health needs. Americans have more medical visits than dental visits annually. In 2019, about 37 percent of Americans had a medical visit and a dental visit, 33 percent had a medical visit only, 21 percent had neither a medical visit nor a dental visit, and 9 percent had a dental visit only.6 Fragmented care delivery continues to characterize much of the health care system in the United States (US). The resulting inadequate access to care for many people, in addition to poor care coordination among health care professionals, exacerbates poor health outcomes and contributes to health disparities.7 One solution is integrating DHs into primary care settings to increase access to oral health care, in particular for individuals who face barriers accessing the traditional oral health care system, such as pregnant people.
Pregnancy is a unique period that is characterized by complex physiological changes, which may adversely affect oral health. Pregnant people need access to oral health care to have the best possible oral health and overall health. In Michigan, only about 20 percent of pregnant people with low incomes received oral health care in 2021.8 This case study describes a program that integrates DHs into obstetrics and gynecology (OB/GYN) clinics in federally qualified health centers (FQHCs) located in underserved areas of Michigan with the goal of improving the oral health of pregnant people.
CASE DESCRIPTION
In 2018, the Michigan Department of Health and Human Services’ (MDHHS’) Medicaid program awarded a $1 million grant to the University of Detroit Mercy School of Dentistry to develop and implement a pilot program to improve access to oral health care for pregnant people with low incomes. The program, Michigan Initiative for Maternal and Infant Oral Health (MIMIOH), was led by a multi-agency project team composed of the MDHHS Oral Health Program, the Michigan Primary Care Association, and the University of Detroit Mercy School of Dentistry. The project team selected six geographically diverse FQHC pilot sites via a competitive application process. The program focused on replicating a successful model of integrating full-time DHs into OB/GYN clinics. This model has been successfully implemented since 2014 at Grace Health, a FQHC in Battle Creek, Michigan. A key facilitator for the MIMIOH was Michigan’s Public Dental Prevention Program (PA 161 Program) that permits collaborative practice with indirect supervision of DHs by dentists to allow preventive oral health care for unassigned (i.e., without a dental home) and underserved people. Participating MIMIOH FQHCs were required to apply for the PA 161 Program and were subject to reporting and associated rules and regulations. As of 2021, Michigan is one of 42 states that allows people to receive oral health care directly from DHs without the specific authorization of a dentist.9
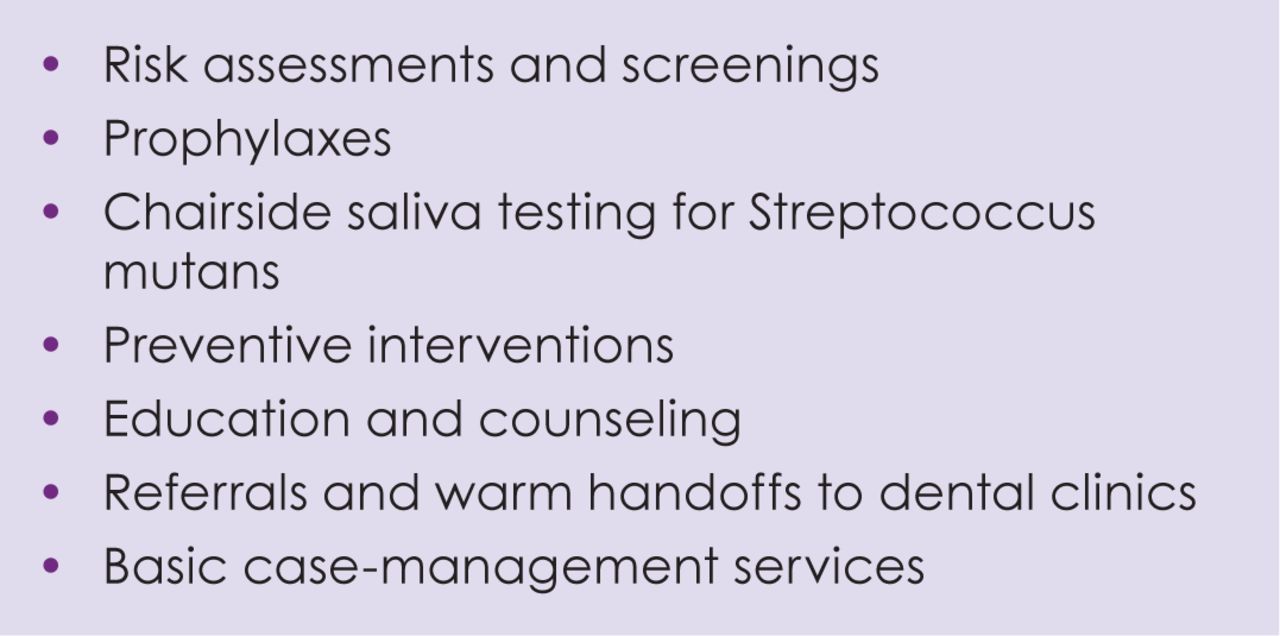
Each of the six participating FQHC sites hired a full-time DH to integrate into the prenatal care team and installed a dental operatory within its OB/GYN clinic. The MIMIOH initially funded the DH salaries, equipment and supplies for dental operatories in addition to oral health supplies and educational resources for patients at the sites. Dental hygienists provided a range of oral health care services (Figure 1), including during CenteringPregnancy visits, a model that brings together pregnant people with similar due dates in a comfortable group setting for prenatal care.10 The goal was for the DH to see each pregnant person at least once per trimester and for a postpartum visit; however, many patients faced socioeconomic barriers that delayed initiation of prenatal care, and some appointments were missed. Therefore, the DH provided oral health care to pregnant people whenever possible, including while they waited in an exam room or the waiting room for an appointment with their prenatal care health professional. For OB/GYN clinics that had a co-located dental clinic in the same building, the DH provided warm handoffs to the dental clinic for patients with urgent treatment needs. The program was marketed as a standard part of prenatal care at the participating FQHC sites, although at the start of the program, patients had the option to decline oral health care. In some cases, fear of oral health care and previous trauma contributed to patients’ reluctance to see the DH.

Oral health care services provided by dental hygienists in OB/GYN clinics
As MIMIOH progressed, opportunities to replicate the model emerged. In 2019, with an additional $640,000 in funding from the Delta Dental Foundation, the project expanded to an additional three FQHCs while continuing to support the original six sites. To sustain the program, OB/GYN clinics needed a sufficient number of patients (at least 200 prenatal patients annually) and to provide enough oral health care to justify the DH’s salary. Clinics also had to consider whether billed encounters would reflect the amount of time required for the DH to provide comprehensive dental hygiene care to pregnant people. The methodologies used to calculate whether the program was financially sustainable differed by each FQHC, but typically included oral health care provided by the DH integrated in the OB/GYN clinic and oral health care (e.g., restorative care) for pregnant people referred to the FQHC’s dental clinic. In some FQHCs, the DHs split their time between pediatric and OB/GYN clinics, which factored into the financial sustainability of the model.
Before the onset of the COVID-19 pandemic, there were nine FQHC sites with DHs integrated in OB/GYN clinics. All clinics experienced disruptions to their MIMIOH activities due to the pandemic, and some completely ceased activities if the DHs were reassigned to work in dental clinics or to other roles within the FQHCs because of workforce shortages or for other reasons.
RESULTS OF THE INTERVENTION
The Susan B. Meister Child Health Evaluation and Research (CHEAR) Center at the University of Michigan helped document trends in health care and oral health care for pregnant people enrolled in Medicaid and conducted key informant interviews with 36 oral health, prenatal, and administrative staff from participating MIMIOH sites. Interview participants consistently mentioned four key elements of successful MIMIOH implementation. First, DHs must want to work in public health settings and be able to function flexibly without a set schedule. Identifying DHs with desirable characteristics (e.g., upbeat, encouraging) for a fast-paced, integrated clinic is essential. Second, buy-in from prenatal health care professionals is critical and includes understanding the importance of oral health care for pregnant people as well as the importance of providing that care. Third, clinical workflows must facilitate contact between the DH and pregnant people and be structured, but not rigid, as prenatal appointments often run long and involve multiple clinical staff members. Fourth, oral health care should be presented as a standard part of prenatal care and not as an extra or optional service. Several FQHC sites offered oral health care as optional initially and found that pregnant people were reluctant to accept care from the DH; however, acceptance improved after sites revised their descriptions of the program. In addition to these key elements, having the OB/GYN clinic and dental clinic co-located within the same building provides opportunities for warm hand-offs and increases the likelihood of follow-up oral health visits for patients referred to the dental clinic for care. There was also broad agreement that integrating DHs in OB/GYN clinics requires funding and prioritization within the host organization, particularly for startup costs.
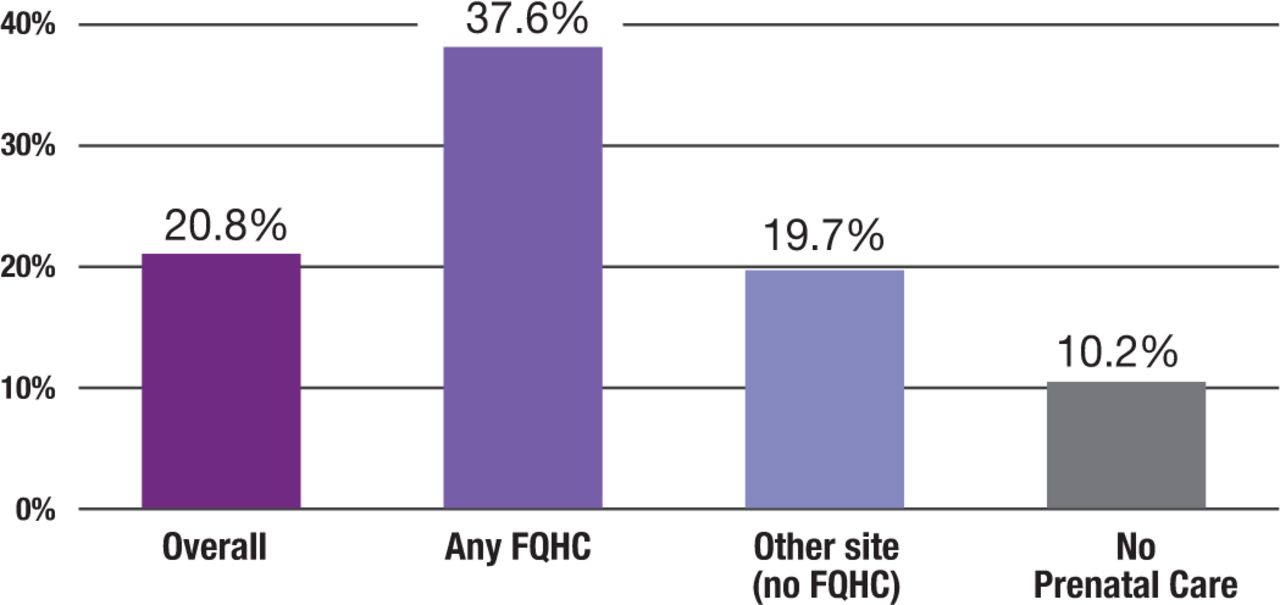
The CHEAR Center also conducted a comprehensive Medicaid data analysis of the program. The study population included Medicaid beneficiaries in Michigan with a live birth delivery between April 1, 2018, and December 31, 2020. Findings showed that the percentage of pregnant people receiving oral health care who were also receiving prenatal care at an FQHC (37.6 percent) was nearly double the percentage of those receiving prenatal care at a non-FQHC site (19.7 percent). In addition, the percentage of pregnant people receiving oral health care who were receiving prenatal care at an FQHC (37.6 percent) was nearly four times the percentage of those receiving no prenatal care (10.2%) and nearly two times the percentage of those receiving prenatal care overall for FQHC and non-FQHC sites (20.8%) (Figure 2). Data collected by CHEAR also determined whether MIMIOH participation affected the percentage of pregnant people receiving oral health care at participating FQHCs vs. non-participating FQHCs and found that the percentage of pregnant people receiving oral health care increased at MIMIOH sites when the program was being implemented. In fact, the percentage of pregnant people receiving oral health care increased by nearly 20% in participating FQHCs.

Provision of any type of oral health care by prenatal care site
DISCUSSION
This case study describes an innovative program with DHs integrated in FQHC OB/GYN clinics to provide oral health care to pregnant people. The MIMIOH program helped bridge the divide between prenatal care and oral health care for pregnant people in underserved areas of Michigan. Informant interviews revealed key factors to successfully integrating DHs into OB/GYN clinics, with the selection of DHs with personal characteristics desirable for integrated-care delivery identified as being paramount. In addition, designing appropriate clinical workflows, gaining buy-in from prenatal health care professionals, presenting oral health care as an integral component of prenatal care, having co-located OB/GYN and dental clinics, and maintaining adequate funding were all critical to program success. Analysis of Medicaid data showed that the model increased the percentage of pregnant people receiving oral health care at co-located FQHC dental clinics. This finding highlights the value of integrating DHs into primary care clinics in public health settings like FQHCs to increase access to oral health care for those who might otherwise not receive care. Unfortunately, the COVID-19 pandemic imposed significant constraints on the MIMIOH program, and six of the nine FQHC sites stopped participating. The remaining three sites have continued implementing the model in their OB/GYN clinics.
Dental hygienists provide oral health care in a variety of non-traditional settings such as schools, community-based programs, hospitals, outpatient clinics, long-term care facilities, and pediatric and prenatal medical clinics. Innovative programs such as MIMIOH add to the evidence that integrating DHs into primary care settings can increase access to oral health care, especially for those who face difficulties accessing the traditional oral health care system. This program demonstrates the potential for DHs to leverage collaborative practice agreements and remote supervision in order to increase access to oral health care for pregnant people. Additionally, providing DHs with autonomy to practice to the highest level within their scope of practice and permitting direct Medicaid reimbursement for DHs (currently only 19 states allow Medicaid to reimburse DHs directly11) would make oral health care more accessible for underserved populations, including those with low incomes, those who are members of racial or ethnic minority and other marginalized groups, those residing in dentally underserved areas, and individuals with developmental or acquired disabilities.
CONCLUSIONS
Dental hygienists are well positioned to be integral members of primary care teams to address the oral and systemic health needs of the public. The MIMIOH program demonstrates the impact of integrating DHs into OB/GYN settings on improving access to oral health care for pregnant people. As health care delivery in the U.S. continues to evolve to be more person-centered, team-based, and prevention-focused, DHs have significant potential to improve access to health care and health outcomes in non-traditional settings, particularly for those who are less likely than others to have optimal access to high quality oral health care.
ACKNOWLEDGEMENTS
The authors would like to acknowledge the University of Detroit Mercy School of Dentistry and Professor Divesh Byrappagari for their administrative oversight and management of the project; the Susan B. Meister Child Health Evaluation and Research (CHEAR) Center at the University of Michigan and their team Sarah Clark, Lisa Cohn and Dianne Singer, for their evaluation of the project; and the Delta Dental Foundation for their generous support of the project. We would also like to thank Ruth Barzel and Katrina Holt from the National Maternal and Child Oral Health Resource Center for their review of this manuscript.
Footnotes
NDHRA priority area: Population level: Health services (interventions).
- Received April 17, 2023.
- Accepted May 6, 2023.
- Copyright © 2023 The American Dental Hygienists’ Association





{kind=link}
{kind=link}