



Abstract
Purpose: Limited scleroderma is associated with significant risks to the orofacial complex. The purpose of this mixed methods study was to investigate the experiences of participants with limited scleroderma related to oral health quality of life and oral health.
Methods: A sequential mixed methods study was used in a population of individuals diagnosed with limited scleroderma. Participants were recruited through rheumatology specialists, referral, and social media; purposive sampling was used to recruit participants to be interviewed. The validated Oral Health Impact profile (OHIP) and Mouth Handicap in Systemic Sclerosis (MHISS) instruments and semi-structured interviews were used for data collection. Quantitative data were analyzed using descriptive statistics and the qualitative data were reported through thematic analysis.
Results: Forty-eight (n=48) qualifying participants participated in the quantitative phase, and 12 (n=12) participated in the qualitative phase. Based on a Likert Scale from 0-4, mean OHIP-14 scores ranged from 2.76 to 2.85, with anxiety over oral condition, embarrassed by oral problems, and oral self-consciousness having the greatest negative impact on quality of life. Mean MHISS scores ranged from 2.13 to 3.11. The highest OHRQoL scores were related to dry mouth symptoms. Factors influencing oral health-related quality of life were varied; dry mouth and microstomia were the prevalent complaints. Thematic analysis revealed challenges to oral health included self-care and professional dental care factors, both of which depended upon individual disease expression. Financial and emotional burdens also influenced participants’ oral health.
Conclusion: The oral health-related quality of life of those with limited scleroderma is impacted by multiple factors and oral health care professionals must seek out improved treatment modalities to address the needs of these vulnerable individuals. Future studies related to interprofessional collaborative care with scleroderma specialists are recommended.
- systemic scleroderma
- limited scleroderma
- CREST syndrome
- oral health-related quality of life
- autoimmune disease
- patient experience
Introduction
There are two major categories of scleroderma, an autoimmune disorder, limited and diffuse. Diffuse scleroderma has widespread skin involvement, rapid progression, and early visceral involvement.1 Limited cutaneous systemic scleroderma [lcSSc], or limited scleroderma, is considered to be a rare autoimmune condition1-7 and was formerly known as CREST syndrome. The term “CREST” is an acronym for the associated clinical features combining five autoimmune conditions including the following: Calcinosis cutis, Raynaud’s phenomenon, esophageal dysmotility, sclerodactyly, and telangiectasia.2,8-10 Limited scleroderma patients may present with some or all of the five classic presentations.
Limited scleroderma is a slowly progressing disease with a female to male ratio of 5:1 and mean age of 55.3,5 Of the various types of scleroderma, 80% of those diagnosed with limited scleroderma test positive for the anticentromere antibody.11 Several studies reported the prevalence of scleroderma worldwide.12-14 A current review of the literature found rates of 150-300 cases per million for Europe, the United States, Australia, and Argentina.14 Lower prevalence rates of 31-88 cases per million were found in Scandinavia, Japan, the United Kingdom, Taiwan, and India.14 Diagnosis of limited scleroderma is difficult because it mimics multiple conditions.10 There are new, promising studies exploring the possibility of early diagnosis of scleroderma through salivary testing.15-16 Given the difficulty in diagnosis, identification of salivary biomarkers in scleroderma may provide a way for early diagnosis and even a possible way to distinguish between systemic and limited forms. More studies are required before conclusive diagnoses can be made using these biomarkers.16
Limited scleroderma often manifests with clear orofacial signs and symptoms. Due to vascular, inflammatory and fibrotic changes associated with the disease, the head and neck regions are susceptible to the effects of gastroesophageal reflux disease [GERD], vasoconstriction, fibrosis, hemorrhage, limited opening (microstomia), increased incidence of periodontal disease, and xerostomia.2,3 Early signs of the disease might include trigeminal neuropathy with no clinical cause, or persistent GERD, resulting in acid erosion, dentin hypersensitivity, and mucogingival paresthesia.2,17,18 The tightening of the skin around the hands and orofacial structures impact oral self-care performance and movement of oral structures. These factors contribute to an overall increased risk of oral disease.18,19 Fibrotic changes in oral tissues may lead to gingival recession and loss of gingival attachment. Tissue hardening may be evident in the tongue and soft palate.20 The lack of sufficient self-care, limited mouth opening, and decreased vascularization are implicated in an increased incidence and risk of periodontitis in patients with limited scleroderma.17
The debilitating oral symptoms related to limited scleroderma affect the quality of life of the sufferers. Oral Health-related Quality of Life [OHRQoL] is associated with functional factors, psychological factors, social factors, and the experience of pain or discomfort, and is a highly individual concept. This construct can also measure treatment efficacy compared with adverse effects of a disease, help identify needs of those with specific diseases, and aid providers in monitoring patient status and in making treatment decisions.21 Assessment of OHRQoL is accomplished by comparing individuals’ expectations with their actual experiences.22 Published literature have established that OHRQoL is impacted in patients with scleroderma.23,24
In systematic reviews on systemic scleroderma, health-related quality of life was explored in these populations. While these reviews focused on both physical and mental impairment, none were related to oral health.21,25 Cross-sectional studies conducted by the Canadian Scleroderma Research Group Registry demonstrated impaired OHRQoL among scleroderma participants.23 This same group also determined that OHRQoL is independently associated with health-related quality of life.26 Literature shows a high correlation between OHRQoL and the manifestations of orofacial symptoms in individuals with scleroderma but fails to report participant experiences with the limited form of the disease. Qualitative studies in the literature provide some insight into participant experiences with systemic scleroderma and chronic disease, although none found are specific to oral health. Any orofacial symptoms found in study participants were reported as being present with very little discussion as to the effect on their OHRQoL.
Limited scleroderma is associated with significant risks to the orofacial complex, yet patients with connective tissue diseases are less likely to seek continuing oral health interventions.27 Though there have been case studies published about limited scleroderma and quantitative studies specific to systemic scleroderma, there are no known qualitative studies that focus on participant experiences regarding oral health. Most studies in the literature have focused primarily on the systemic form of scleroderma, possibly due to its rapid progression and high morbidity and mortality rates.23 Additionally, research has shown a lower oral health-related quality of life, and yet a reduced likelihood to seek professional oral health services for this population. However, the reasons for this disparity are unclear. Researchers who have conducted qualitative studies related to scleroderma and chronic disease have reported a limited discussion of orofacial symptoms as simply being present and very little discussion as to the effect these changes have on the participants, other than effects on self-esteem.28 Recently studies related to scleroderma demonstrated a low oral health - related quality of life among these participants.23,24 However, few studies solely describe the limited form of scleroderma and the impact on oral health-related quality of life. The purpose of this study was to investigate the experiences of participants with limited scleroderma related to their oral health and the impact of the disease on their ability to seek professional oral care.
Methods
A sequential mixed method research approach was selected for this study. The Institutional Review Board, Human Subjects Committee of the Idaho State University approved this study and assigned the protocol number IRB-FY2016-342. To answer the question regarding the oral health related quality of life of individuals with limited scleroderma, quantitative data were generated through use of the reliable and validated instruments Oral Health Impact Profile (OHIP-14) short form, and the Mouth Handicap in Systemic Sclerosis Scale (MHISS).29-31 The OHIP-14 short form is a scaled index of the social impact of oral disorders which draws on a theoretical hierarchy of oral health outcomes, designed for clinical use. The questionnaire was developed to measure people’s perceptions of the impact of oral conditions on their well-being.29,30 The MHISS was developed to assess mouth disability in scleroderma patients. It is useful to evaluate handicaps related to the mouth and face because it is simple, easily understood and not time-consuming.31,32 Using both instruments for future studies related to the oral health of scleroderma individuals has been recommended in previous research.23 The instruments were used in their original forms with Likert scales, and combined into one instrument for ease of administration and permission was granted to use both instruments. Two items related to demographic and diagnostic information were added pertaining to ability to perform oral care tasks and ability to seek professional oral care. These items were directly related to the research questions thereby demonstrating content validity.
The convenience sample for the quantitative phase consisted of persons diagnosed with limited scleroderma who were recruited primarily through social media. Snowball sampling provided additional participants as individuals informed others of this research opportunity.
Individuals who consented to participate were provided detailed instructions and a link to complete the online questionnaire. The OHIP-14 was scored on a scale of 0-4 with 0=never, 1=hardly ever, 2=occasionally, 3=fairly often, 4= very often. Mean scores were derived for this scale. A low mean score indicated participants largely reported the experience rarely occurred, while a high score indicated the experience occurred very often. The MHISS was scored on a similar scale in which 0=never and 4=always. Therefore, a high score on the MHISS indicates the experience always occurred. The quantitative data were downloaded into a spreadsheet (Excel, Microsoft, Bellevue, WA) and analyzed using descriptive statistics.
A qualitative inquiry was implemented to answer the question regarding the experiences related to oral health and oral health care of an individual with limited scleroderma. Results of the quantitative questionnaire allowed investigators to identify participants displaying orofacial disease symptoms who were contacted for the qualitative phase of the study. For the purpose of generating information-rich data, only participants who reported low oral health-related quality of life were considered and were recruited as the purposive sample.
Qualitative research in the form of interviews were used to elicit data regarding the oral and general health experiences of diagnosed individuals. Informed consent procedures were completed before implementation of the semi-structured interviews via telephone or video conferencing. Participants were sent the interview guide at least one week before data collection to help them formulate responses to the interview questions. The interview guide consisted of five, broad questions related to oral health experiences. As the study progressed, more specific questions were added to gain more depth and breadth to the data generated and the questions were created to address gaps in current literature. Pseudonyms replaced participant names during the interview and on the transcripts to preserve confidentiality and anonymity. Each interview was recorded, transcribed verbatim, and verified by the principal investigator (PI) for accuracy prior to data analysis. Field notes were collected during the interview and throughout the data collection process to capture characteristics of the participants in the interview setting, as well as to record thoughts, perceptions, and ideas of the PI.33
Open coding was used to deconstruct the data into small segments followed by axial coding to combine these segments into larger categories or themes; this process occurred after each interview. The researchers used the constant comparative method to compare open codes and categories after each interview to ensure consistency in data analysis. Additional methods to ensure the credibility (validity) and reliability of the analysis included a co-investigator who fulfilled the role of inquiry auditor. The inquiry auditor ensured that investigator bias did not influence the data analysis and verified emergent themes and conclusions.33 Member checks were conducted by sending the preliminary data analysis to each participant and asking them to review it for accuracy. This step served to control for misinterpretation of participant perspectives and reveal any investigator bias.33 Participants’ comments were documented as part of the study, along with the actions taken by the PI in response to their suggestions.
Results
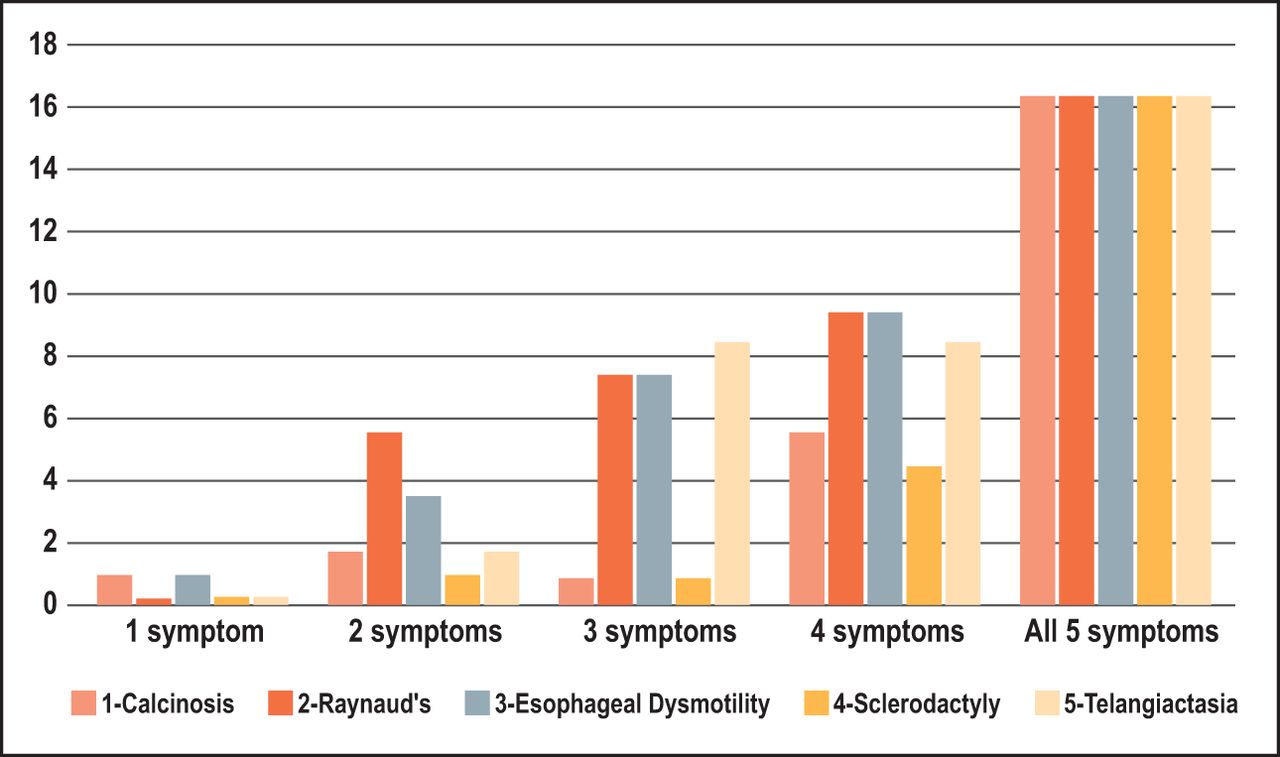
Forty-eight individuals with limited scleroderma from the United States, Canada, Australia, and New Zealand completed the quantitative online questionnaire. Most participants were middle-aged females and identified as white/Caucasian (Table I). Each participant indicated the presence of at least one CREST syndrome symptom, however most indicated the presence of multiple (3-5) symptom presentations (Figure 1). Most participants (n=34, 68%) were diagnosed with limited scleroderma through a blood test, while 28% (n=14) were diagnosed by the presence of CREST syndrome-related disease presentations and 4% (n=2) were unsure of their method of diagnosis. Participants had experienced the symptoms from one to fifty years, with the greatest percentage of individuals (36%, n=18) living with the disease for 11-20 years.
Demographics*

Number of limited scleroderma presentations present in each subject (n=48)
Results of the OHIP-14 indicated that respondents reported a range of difficulties related to oral health as presented in Table II. Oral self-consciousness (n=15, 33%) and anxiety over oral condition (n=10, 22%) were symptoms occurring more frequently. Based on a Likert Scale from 0-4, mean OHIP-14 scores ranged from 2.76 to 2.85, with anxiety over oral condition, embarrassed by oral problems, and oral self-consciousness having the greatest negative impact on quality of life: participants who selected “don’t know” were not counted in mean scores. Results of the MHISS Scale indicated that dry mouth (n=18, 38%), the need to drink often (n=19, 40%), and avoidance of certain beverages (n=15, 32%) were always a concern. Mean MHISS scores ranges from 2.13 to 3.11. The highest OHRQoL scores were related to dry mouth symptoms, with 3.00 and 3.11 mean scores, respectively. Additional questions were asked regarding difficulty performing oral hygiene tasks and seeking professional oral care, showing mean scores of 2.58 and 2.64, respectively.
Oral Health Related Quality of Life by symptom/complaint; combined OHIP and MHISS instruments* (n=48)
The qualitative findings provided a deeper exploration of the experiences of limited scleroderma persons related to oral health quality of life and oral health. Twelve participants completed interviews, lasting between 30 and 45 minutes. The major themes to emerge from the data analysis included: challenges and adaptations associated with oral self-care, challenges and adaptations associated with professional oral care, emotional and financial burden, and suggestions from respondents to improve professional oral care. Each theme is described in detail with supporting quotes in Table III.
Additional Quotes from Study Participants
Challenges and adaptations associated with oral self-care
One challenge experienced by the participants was pain associated with self-care, especially in times of disease exacerbation. “Eating…even brushing my teeth is painful at times. When I am in a flare, I can’t hardly brush my teeth.” When one participant became bed bound, her daughters helped her adapt to the situation by preparing for completion of her daily routine in bed. Another challenge to self-care was decreased hand dexterity and strength related to the scleroderma symptoms. Adaptations to overcome these challenges included the use of a power toothbrush, various types of flossers and a water flosser. One strategy was to leave the toothpaste and mouth rinse caps loose to ease the access to these products. Additional quotes are shown in Table III.
Another commonly reported challenge was the tightening of the buccal mucosa and a minimal mouth opening. Participants modified their self-care routine by using a toddler toothbrush, interproximal brushes and power toothbrushes. Additionally, one participant only flossed her anterior teeth due to the limited access to posterior teeth. Ulcerations on the fingers hindered flossing; therefore, flossing sticks were more easily manipulated than floss.
Oral sensitivity due to tooth pain, neuralgia, mouth sores, and xerostomia was problematic for daily self-care for the participants. Modifications to reduce tooth sensitivity were using a prescription strength fluoride toothpaste, an over-the-counter (OTC) sensitivity toothpaste and avoiding rinsing with cold water. Oral products with mint flavor and alcohol seemed to aggravate the oral mucosa; therefore, natural toothpaste and baking soda were replacements. Alternatives to commercial mouth rinses were warm saltwater and a mixture of peroxide and water.
Xerostomia was a very common oral challenge among the participants. Various products designed to alleviate these symptoms such as OTC oral lubricants, mouth rinses and lozenges were used. While some participants experienced relief from these products, many had tried multiple products with no success.
Challenges and adaptations associated with professional oral care
Minimal mouth opening was a challenge to completing intraoral procedures requiring instrumentation and exposure of bitewing and periapical radiographs. Bite blocks held the mouth open but were uncomfortable and even painful. One participant was referred to another office to have a panoramic radiograph exposed, as other intraoral images were impossible due to limited opening. Other reported adaptations were the use of pain relief medications prior to dental appointments and pediatric-size instruments. Dry mouth and lips influenced participant comfort in the dental office, as well as oral health. Participants attributed the high incidence of dental caries and tooth loss to xerostomia and difficulties with professional oral care. Modifications included the use of lip balm to keep the lips lubricated to assist in opening the mouth and more frequent re-care visits to prevent oral diseases.
Financial and emotional burden
While frequent re-care intervals were recommended due to disease risks, this recommendation also contributed to financial burden. Participants adapted to the cost by not following the oral health professionals’ recommendations for more frequent care or opted for a less expensive alternative treatment.
Participants also reported difficulty in finding oral healthcare providers who had knowledge of scleroderma. A major challenge for those with limited scleroderma is general pain with professional dental care, which has a negative emotional impact. Additionally, many experienced a lack of empathy and understanding among oral healthcare professionals. Furthermore, participants reported that the oral effects of limited scleroderma negatively influenced their self-esteem.
Suggestions to improve professional oral health care
Participants provided many suggestions to improve professional oral health care for individuals suffering with limited scleroderma. These individuals found that they needed to educate healthcare professionals about their disease. Much of their time was spent discussing disease basics, rather than their own experiences with scleroderma. From their perspective, many healthcare providers did not give credence to their experiences with this often-invisible disease. The desire of this vulnerable population was that their oral healthcare providers be willing to learn about individual disease experiences and expressions. Participants reported that dental hygienists were knowledgeable in recommending products to alleviate some oral symptoms and valued individualized oral health instructions addressing issues related to scleroderma.
Participants expressed the desire for interactions with providers who listened to and believed them. Additionally, suggestions included the need for compassion, direction, and understanding from their oral healthcare providers. Some had experienced the opposite as expressed by Marcia. “Dental wise, I have very vivid memories of going to a new dentist who screamed at me because I couldn’t open my mouth large enough. I have a very, very small mouth. That is part of CREST.” Others had more positive experiences. “My dentist has just been very patient, and every understanding and I think that is the key. He just doesn’t see me as another patient. He has a lot of compassion, and I think that is really important to find somebody like that.”
Other participants reported successes in treatment, due to patience and perseverance on the part of the provider in finding the best treatments.
“[My dentist] doesn’t want to pull my teeth out…he tries to work with me to see what will best fit me. He lifted my spirits too, because he started to lighten the teeth and fix me up, so I started to have a beautiful smile. He was trying to make me personally feel better. That is one of the compliments I get from most everybody is a beautiful smile.” Hungry Newfie
Participants reported a generalized lack of understanding about limited scleroderma among healthcare professionals. As patients, these participants expressed the need for providers who are willing to learn more about the conditions specifically affecting them. This lack of knowledge about limited scleroderma should be addressed through continuing education courses, and through gaining more experience treating those with scleroderma.
“I know [my dentist] has read about scleroderma and kind of knows what it is … I did refer a couple of other scleroderma patients to her, so she got some other experience with a few that had diffuse scleroderma and really had tight mouth openings and tooth issues. She definitely got real fast education about it when she treated that other patient. But, I think, myself and that other patient are probably the dentist’s only experience with scleroderma.” Jennifer
Participants further recommended providers seek education about the disease through scholarly research and attendance at scleroderma meetings.
Discussion
This study generated information specific to the limited form of scleroderma and documented participant experiences related to oral health, in an effort to contribute to the knowledge about this rare disease. Because individuals with limited scleroderma present with varied disease expressions and often live with the disease for decades, the implications related to professional oral healthcare are important to understand. These findings are supported by epidemiologic data showing that people with the limited form of the disease live with the disease longer than those with the diffuse form.14 This study has documented the disparity between the oral health needs of these participants and the oral care adaptations available to them.
Questionnaire and interview results provided information regarding the oral health experiences of individuals with limited scleroderma, which negatively impacts their oral health-related quality of life. Xerostomia was the most commonly reported complaint, with mixed results being reported in the efficacy of common remedies. Dry mouth negatively influenced both self-care and professional care and contributed to altered dentition through increased dental caries incidence, as well. This increased risk of caries contributed to tooth loss, financial burden, and difficulties seeking professional care. These findings were similar to what has been previously described in the literature.24,26,34-35
Altered dentition and microstomia were also commonly reported by participants, and these oral conditions had a significant impact on their quality of life manifesting through difficulty eating, self-consciousness and self-esteem affectation, difficulty with oral self-care, and difficulty with professional oral care. Very few adaptations were reported as being available to the limited scleroderma participants and the use of smaller instruments and mouth props were only minimally successful in addressing the needs of both provider and patient. It was surprising that none of the individuals interviewed reported the measuring of maximal mouth opening by oral healthcare providers. There is evidence to support the success at increasing maximal mouth opening in scleroderma patients through a regimented exercise program, showing an average 10 mm increase (an approximate 9% improvement) after 18 weeks.19 Therefore, dental hygiene treatment plans that include facial exercises, frequent re-care intervals, abbreviated appointments, new physiotherapy aids or alternate uses of existing aids, and referrals for specialized care, may better meet the needs of individuals with limited scleroderma, a finding supported in the literature.31,36-38
An important finding of this study concerned reasons why individuals with this disease may not seek regular professional oral health care. Some of the themes evident in the qualitative portion of this study provided insight into this issue. Participants reported financial burden, physical limitations, pain with treatment, and lack of knowledge and compassion by oral healthcare providers. Findings regarding financial burden, pain and limitation are supported in the literature.34,35 Participants understand that healthcare providers cannot reasonably have substantial knowledge of every rare disease. These participants highly valued interactions with providers who listened to their lived experiences and expertise (self-knowledge of disease). Most importantly, they admired and sought out providers who were willing to learn more about scleroderma to better serve their needs. Participants specifically appreciated dental hygienists for their role in promoting oral health through product recommendations but noted oral healthcare providers can do still more by developing innovative ways to utilize currently available products, or by creating new products that will better suit their needs. Participant suggestions are summarized in Table IV.
Recommendations for oral healthcare providers
These findings are relevant because current literature does not address these issues specific to limited scleroderma. As a mixed methods study with a limited sample size, these results are not generalizable. However, the goal of qualitative research is not to generalize findings but to generate a sufficient amount of valuable information.33 The sample size for the qualitative study is supported by similar studies, by the sole focus on the limited form, and by the rarity of the disease.39,40
Further research is required to better meet the special needs of individuals with limited scleroderma. There is also a need for the development of better adaptive tools and strategies supportive of effective self-care. Collaboration between dental professionals and other interprofessional providers in scleroderma clinics merits further exploration.
Conclusion
The oral health related quality of life of individuals with limited scleroderma is impacted by multiple factors. This study demonstrated the need for compassion and understanding among oral healthcare providers when serving those with limited scleroderma. To address the needs of this vulnerable population, oral health professionals must seek out improved treatment modalities. The measuring of maximal mouth opening should be part of the dental hygiene process of care for scleroderma patients. Collection of these data along with information regarding other oral manifestations experienced by the patient will allow the dental team to treatment plan appropriate interventions. Future studies related to interprofessional collaborative care between oral health professionals and scleroderma specialists is recommended.
Footnotes
This manuscript supports the NDHRA priority area, Population level: Access to care (vulnerable populations).
- Received June 30, 2020.
- Accepted December 15, 2020.
- Copyright © 2021 The American Dental Hygienists’ Association





{kind=link}