



Abstract
Purpose: Strict eligibility criteria exclude a majority of the veteran population from receiving oral healthcare benefits through the Veterans' Administration Dental Care program (VADC). The purpose of this study was to examine perceptions of oral health status, and access/barriers to dental care of veterans who are ineligible for VADC benefits.
Methods: This cross-sectional study was conducted using a 24-item paper survey, disseminated in person to 227 veterans across the state of Michigan over a period of two months. Items included socio-demographic information, questions regarding perceptions of oral health, access to dental care, and perceived barriers. Descriptive statistics were collected to provide an overview of the data.
Results: A response rate of 80% (n=182) was achieved. Veterans who perceived themselves as having a poor oral health status were less likely to have a dental home (p=.000) or receive dental care (p=.001). Respondents were more likely to report cost as a barrier (p=.000), and to report having had a toothache during the past 12-months (p=.000).
Conclusion: Results from this study indicate that while veterans in general value the importance of oral healthcare, cost and time are significant barriers to accessing dental care for individual's ineligible for VADC benefits. Veterans who perceive themselves as having poor oral health are more likely to report oral health disparities. Further research is needed to impact Veterans Administration policy and decrease oral health disparities.
Introduction
Determinants of oral health are highly dependent upon a wide range of social contexts. Factors such as access to health insurance and geographic location, in turn, are affected by the social contexts of socioeconomic status derived from education and employment. The oral health objectives of Healthy People 2020 identify visiting a dentist in the previous 12 months as the leading indicator of oral health.1 Access to oral healthcare is a significant challenge for a large portion of the United States (U.S.) population, but often more acutely for the veteran population. While in active service, members of the military have universal, and regularly required access to oral healthcare, but upon separation from the military, this access to care ends.2
Approximately 20 million veterans currently reside in the U.S.3 While the U.S. Department of Veteran Affairs (VA) is intended to serve as a safety net, nearly 1.5 million veterans lack health insurance,4 and fewer than half, (9 million) are enrolled in VA healthcare programs.5 While some literature indicates that veterans are more likely to indicate having a primary care provider as compared to civilians, they are also more likely to report their health as being fair or poor.5
Oral healthcare is not included in the VA standard medical benefit package, and eligibility is determined through a strictly defined separate classification system that actually excludes the majority of veterans.7,8 Criteria to qualify for VADC include service-connected compensable oral conditions; service-connected oral conditions that aggravate a service-connected disability; service-connected disabilities rated at 100%, or a 100% unemployable rating; former Prisoners of War (POW); veterans in vocational rehabilitation programs; and individuals receiving VA medical care whose oral conditions complicate their medical condition.7 Within the VA system, dental care for veterans has been noted as being disproportionately distributed to providing services to those 65 and older, thus introducing disparities for the growing younger segment of the veteran population within a system intended to support their healthcare needs.9 When combined with other significant challenges veterans frequently face, disparities in access to oral healthcare for this population become more significant.
Oral Health Risks
Combat exposure and service to country increase a veteran's risk of oral health disparities.10–12 Studies have shown increased prevalence of periodontal disease, decay, and temporal mandibular disorders in combat veterans.10,12 A 2017 survey from the Centers for Disease Control and Prevention (CDC) reported that 61% of veterans had a history of tobacco use while 16% reported being current users.13 One quarter of post 2001 era veterans reported alcohol misuse and 53% reported binge drinking.14 Opioids and psychotropic medications are frequently prescribed to treat the increased prevalence of polytrauma and mental illness diagnosed in veterans.11,15,16 Oral side effects of these drugs frequently include xerostomia, impacting the severity of oral diseases.17,18 Increased risk of oral disease also contributes to the vulnerability of the veteran population, making access to care more significant in terms over overall quality of life.
Barriers
Mental health disorders can be compounded by social comorbidities. The unique military culture encompasses engrained, rigid principles of self-sacrifice, alertness, dress, and attitude can significantly impact a veteran's ability to return to the unstructured world of civilian life.19 Poor physical and mental health have been shown to significantly impact daily activities in the veteran population as compared to the civilian population,5 creating economic and social challenges and elevating the risk for poor oral health.
As in the general population, education and socioeconomic status are significant barriers to oral healthcare. Almost half of uninsured veterans are 45 years old or younger and have a lower level of education as compared to insured veterans.20 This is of significance as many members of this younger veteran generation have inadequate education, training, or experience outside of the military to make them employable for careers offering medical and dental benefits.20 Previously combat deployed veterans may face additional post-military service employment challenges, as research indicates that this group does not have the same opportunities for career development in the civilian sector.21,22
Veterans have been noted to have a more difficult time obtaining employment in general. Veteran unemployment status, 13%, is disproportionate to the general population.13 In addition, unemployment, particularly long-term, has been linked to a general deterioration in health and chronic disease, placing veterans uniquely at risk.22,23 Service-connected disabilities and mental health issues can also become barriers, as employers consider them as potential cost liabilities.22,24 Unemployment also impacts day-to-day functionality. Lack of finances deeply impacts food and housing insecurity, which can be significantly amplified in veterans with physical and mental health disabilities.22
Veterans also comprise a disproportionate percentage (10-33%) of the homeless population in the U.S.; veterans with combat experience are more likely to face homelessness.25 - 27 Literature shows that the lack of access to oral healthcare is ranked in the top three biggest concerns of homeless veterans.28 Moreover, veterans experiencing any of the barriers previously discussed were more likely to report having poor or fair oral health, with financial hardship preventing them from seeking dental care.29
Limited research for veterans' oral healthcare
Research is limited regarding oral health in the veteran population, especially in regard to how non-VADC eligible veterans' access or pay for oral healthcare services. The Veterans' Health Administration (VHA) within the VA is the largest healthcare organization in the country, providing medical care to nearly nine million veterans nationwide.13,5 As a result, there is a vast amount of research regarding veterans' access to healthcare, however, data is limited regarding access to oral healthcare.13 Additionally, little is known regarding veterans' oral health perceptions creating a critical gap in the literature, as oral health perceptions have been shown to influence the receipt of dental care.3 The purpose of this study was to examine perceptions of oral health status, and access/barriers to dental care of veterans ineligible for Veterans' Administration Dental Care (VADC) in the state of Michigan.
Methods
The University of Michigan (U-M) Institutional Review Board approved this cross-sectional study as exempt from oversight (HUM00127688). A convenience sample of veterans (n=227) affiliated with VFW Posts, American Legion Posts, Team Red White and Blue (RWB), the Patriot Guard Riders, and student veterans at Ferris State University (FSU) participated in this study.
A 24-item paper survey was developed. Questions included demographic information (military branch, separation of service, years served, age, and sex), questions related to a service-related disability, eligibility of VA medical care and dental care, and the respondents' ability to independently perform daily personal oral hygiene tasks. Five-point Likert-scale questions assessed perceptions regarding the importance of oral health, including perceptions regarding their own oral health. Additional questions assessed whether the respondent had a dental home, the time frame of the last dental visit and type of appointment, whether the respondent had a toothache in the last 12 months and how it was managed, and questions regarding dental insurance coverage and barriers to care. Two open-ended questions addressed additional dental concerns and comments.
The survey was pilot tested by six subjects; three dental hygiene faculty members, and three veterans who receive medical care at the VA. A feedback form was attached to the pilot survey, and revisions were made based on the feedback. Paper surveys were then disseminated at veteran organizations by the principal investigator over a period of two months. A cover letter explaining the purpose of the study was attached to the survey and served as an informed consent.
Statistical Package for the Social Sciences (IBM SPSS Statistics for Windows, Version 25.0; Armonk, NY) was utilized for data analysis. Frequency distributions, mean, and standard deviations were analyzed to provide an overview of the data.
Results
A response rate of 80% (n=182) was achieved. The age range of respondents was almost equally divided between elderly veterans (65 years of age or older) and non-elderly veterans (18-64 years of age). The majority of respondents (94%) reported being honorably discharged or retired, making them eligible to apply for VA healthcare and service-connected disability ratings. Table I provides an overview of the respondent's demographic information, service connected disability rating, and type of VA healthcare received by veterans.
Veterans' access and funding of dental care
Among the 182 respondents, 80% (n=145) reported that they were ineligible for VADC, with 6% indicating that they have utilized VADC benefits. Of those who did not qualify for VADC, 40% reported that they lacked dental insurance coverage (Figure 1). Of those who reported not having any dental insurance benefits, 38% percent indicated that cost of care has prevented them from receiving dental treatment.
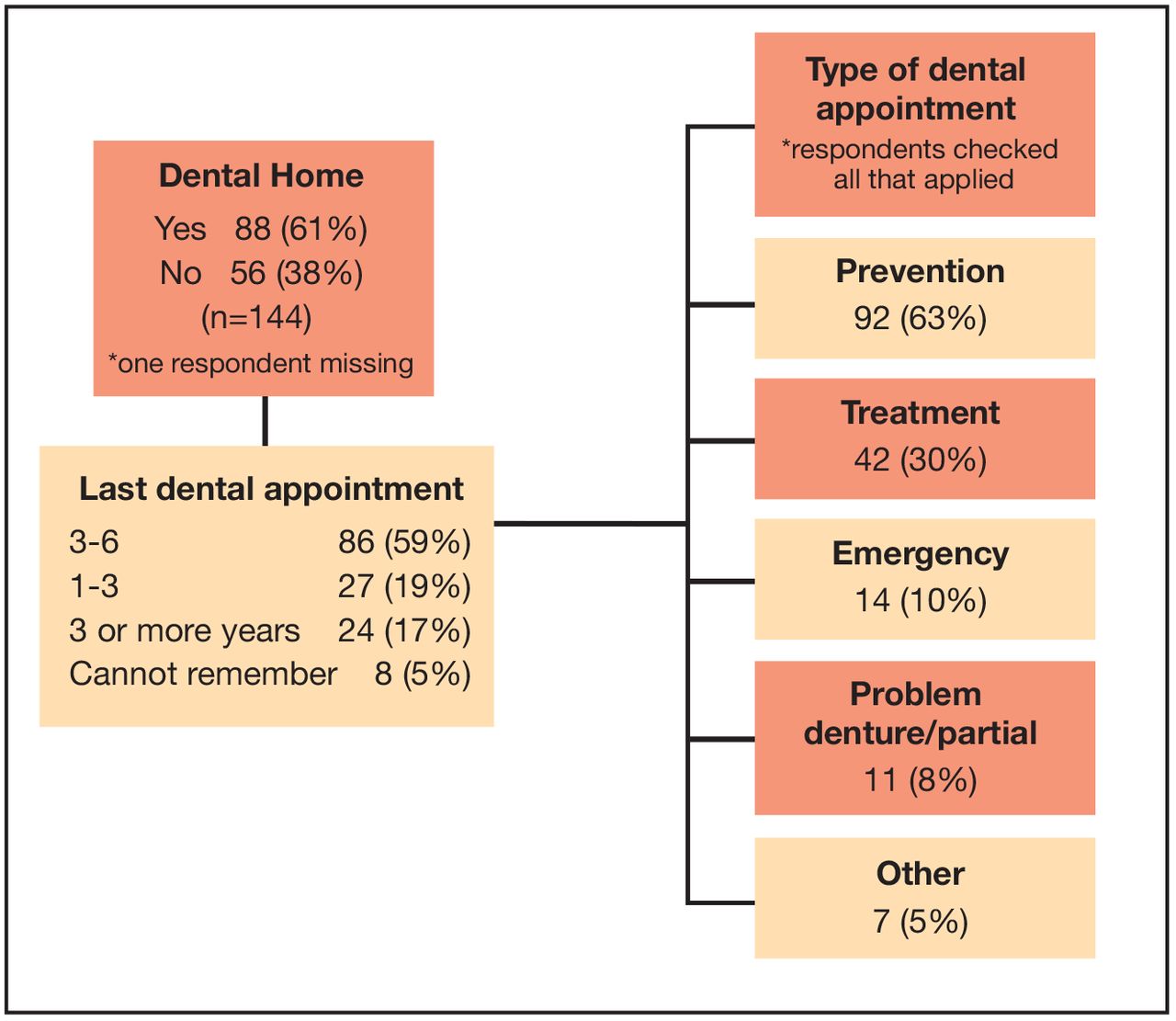
Information regarding dental home, frequency and reason for their last dental appointment is shown in Figure 2. Over half of the VADC ineligible respondents reported having a dental home, and 59% reported having been seen by a dentist in the previous three to six months. However, 17% indicated they had not been seen in three or more years, and 5% could not remember when they had their last dental appointment. Preventive appointments were reported as the most common type of dental appointment followed by treatment, emergency, and problems with a denture or partial.
Sample demographics (n=182)

Dental insurance coverage of veterans ineligible for VADC (n=145)
*respondents checked all dental insurance benefits that applied
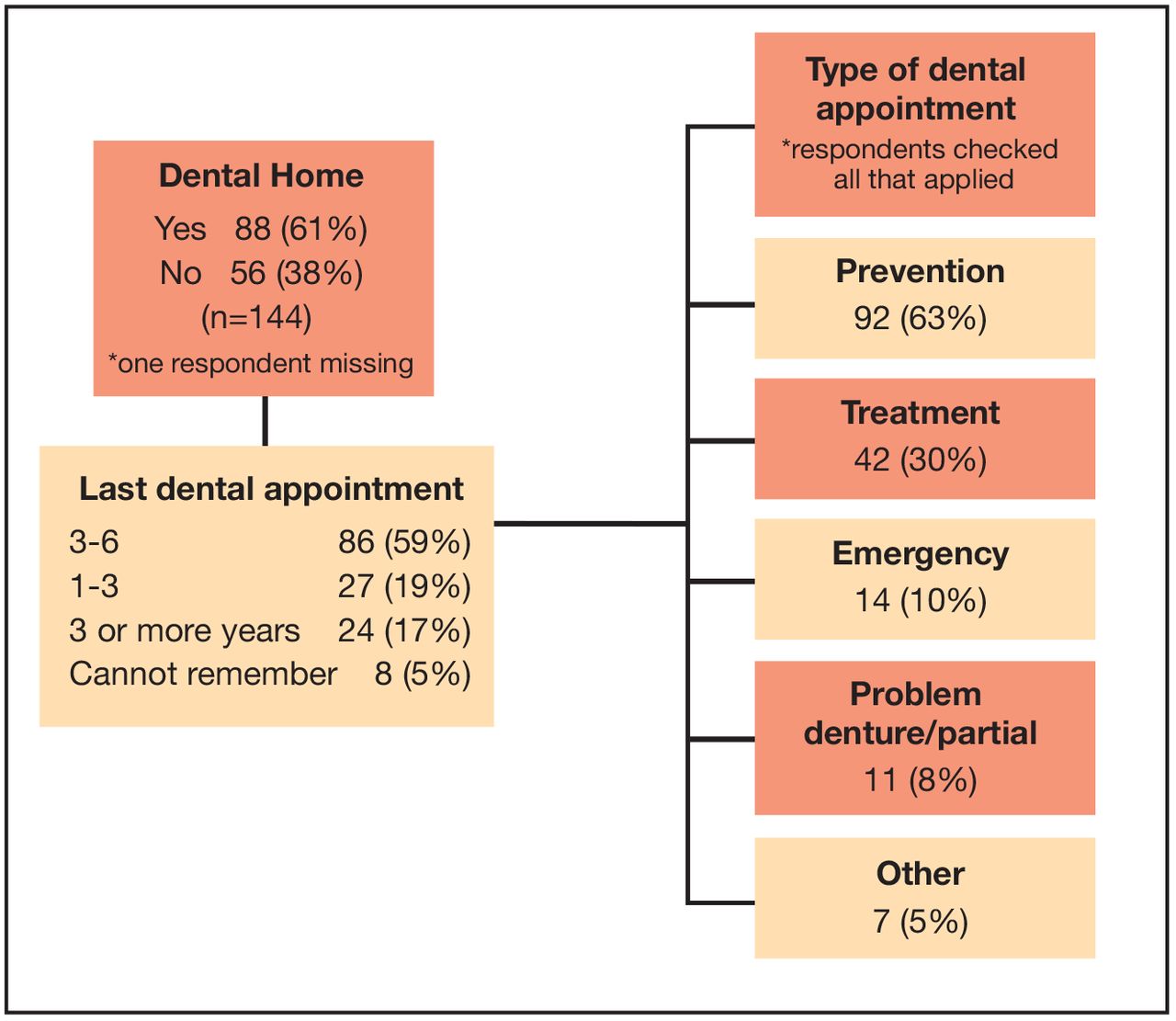
Dental home and appointment description in veterans ineligible for VADC benefits (n=145)
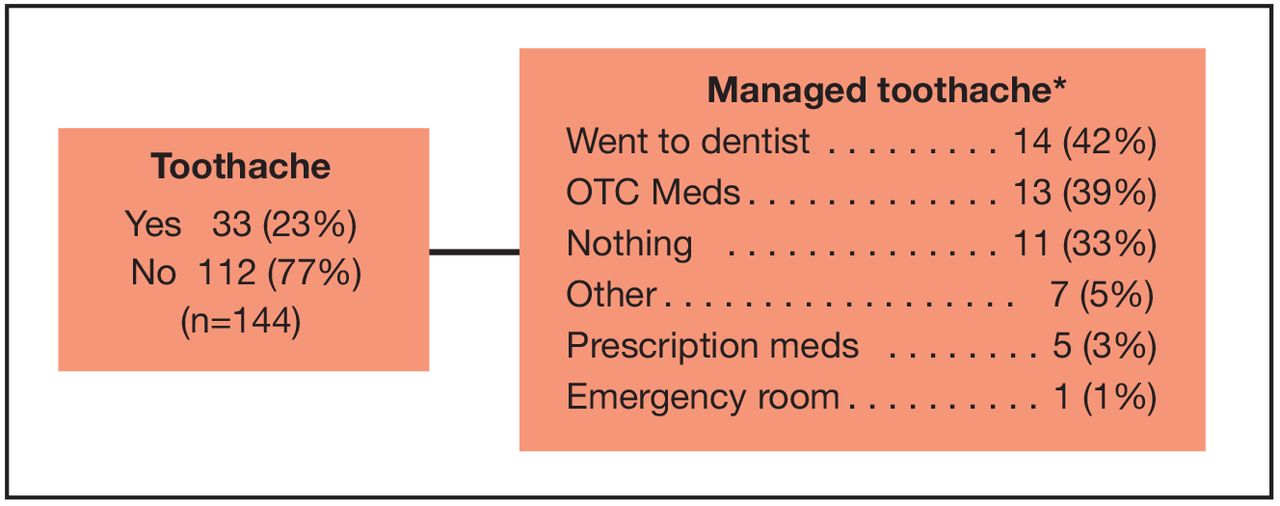
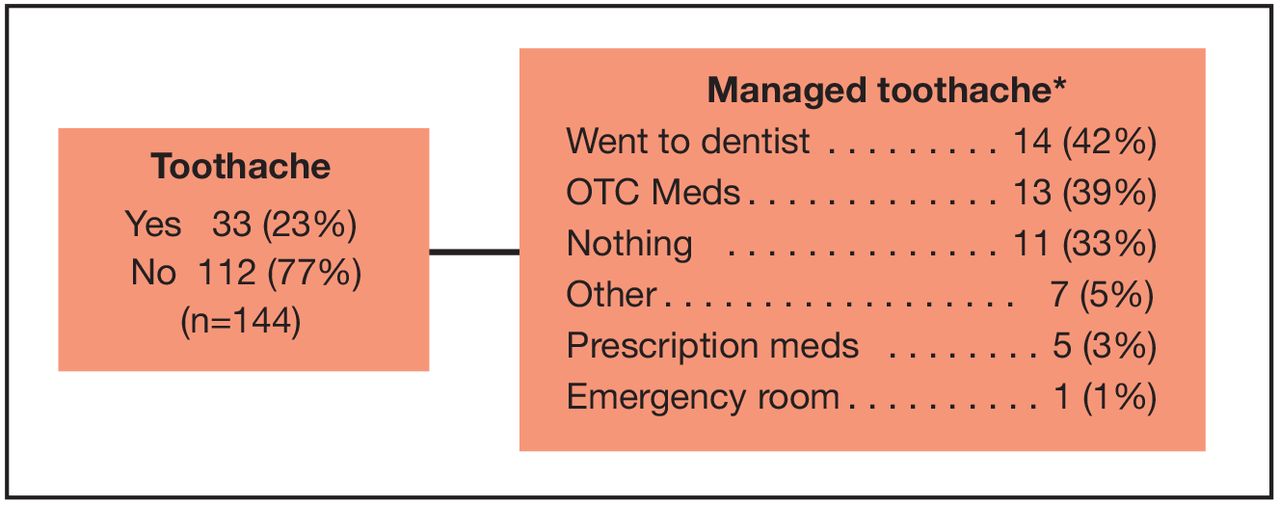
Incidence and management of toothache in last twelve months in veterans ineligible for VADC benefits (n=145)
*Respondents checked all that applied
Frequency and management of toothaches over a twelve-month period for VADC ineligible veterans are shown in Figure 3. Nearly a quarter of veterans reported as having a toothache in the twelve-month period leading up to the study. Less than half (42%) sought dental care, followed closely by those using over the counter medications, or doing nothing at all.
Veteran's perception of oral healthcare
Table II provides an overview of the reported importance of routine dental care and their perception of their own oral health status of VADC ineligible respondents. While the majority (90%) reported routine dental care as important, 25% reported their oral health to be fair or poor. Respondents perceived oral health status as compared to other variables is shown in Table III. Results indicated that lack of dental insurance (p=.161), and self-identified disability ratings (p=.294) were not statistically significant in influencing the respondent's perceived oral health status. Whereas, results did suggest a possible correlation (p=.0.86) between oral health status perception and VADC eligibility status. There was statistical significance in the relationships identified between oral health status perception and lack of dental home (p=.000), a dental visit within the last six months (p=.001), cost inhibiting dental care (p=.000), and whether or not respondents reported having a toothache in the past 12 months (p=.000).
Discussion
Access and funding of oral healthcare
It is well established that there is an access to oral healthcare crisis in the U.S. Determinants of oral health and access to care are significantly influenced by multiple social contexts, however in the veteran population their impact is combined with co-factors including higher rates of mental health disorders, lower education, higher unemployment and homelessness, and a veteran culture that creates additional barriers to access. This study explored veterans' access, funding and attitudes toward oral healthcare.
Respondent demographics in this single state study are representative of national data, making the findings fairly generalizable to the veteran population. Veterans 65 years of age or older and those classified as non-elderly veterans (age 19-64) were relatively equally represented (54% vs. 46%), and is reflective of the rapidly growing, non-elderly segment of the veteran population found in the literature.32 Nearly half of the respondents should qualify for medical care through the VA healthcare system for their service-connected disability. Findings from this study were divergent from the literature, where only one third of all veterans are reported to receive care through the VA.27 Based the qualification criteria for VADC services, findings from this study evaluated and confirmed that the majority of veterans are ineligible for VADC benefits.
Perceived importance of routine dental care and oral health status. Veterans ineligible for VADC benefits (n=145)*
Identifying whether a veteran has declared service-connected disabilities has significant implications. Veterans may be reluctant to report service-connected disabilities which may ultimately increase their VA eligibility due to the often overlooked and misunderstood unique culture of the military. Military healthcare providers are required to report conditions in the military's best interest over the patient's, creating a distrust of healthcare providers that often carries over into civilian life for veterans.33 Additionally, this rigid culture frowns on perceptions of being portrayed as weak or inferior, and embraces a warrior mentality that can have significant impact on veterans' accessing care34 and non-reporting of a service-connected disability has been shown to be more prevalent among uninsured veterans.35 This culture is concerning considering the wide range of reported service-connected disability ratings in this study that were below the required disability rating for VDAC eligibility. Failure to report service-connected disabilities prevents veterans from being accurately rated for disability and potentially excludes them from qualifying for health and dental benefits through the VA.
Veteran's perceived oral health status (n=181)
Eligibility for insurance benefits does not necessarily translate into better health for this veteran population. Veterans may state that they value and access care services but are more likely to report their health as being fair to poor.6 Additionally, it has been noted that veterans can be hesitant to seek out care for fear that their providers will report to their employer.33 The veteran culture and identity might therefore be a significant barrier to accessing oral healthcare. Providers should apply the same principles of cultural competency to veterans as with other cultural groups. Future studies are needed to explore whether or not lack of cultural competence of providers, finances, physical disabilities, or mental illness influence veterans utilization of VADC benefits.22,25
Healthy People 2020 equates a visit to the dentist in the previous 12 months as a leading indicator of oral health.1 While 59% of the respondents reported having had a dental visit in the previous year, over 40% are not meeting this benchmark for oral health. It is important to understand the potential, perceived and actual barriers for access to oral health care in the veteran population and the impact of the cultural taboo of seeking treatment for health needs should be considered. Veterans have a distinct culture of self-sacrifice that conflicts with putting one's own needs first, which can become a barrier to accessing care, even when there is an acute need.33,34
While 20% of veterans qualified for VADC, the majority of those who qualified reported that they did not utilize their benefits. These findings conflict with the majority of veterans who indicated that they perceived the importance of good oral health. However, a significant number of respondents in this study actually rated their own dental health as “fair” or “poor” in spite of reporting having a dental home for routine dental care, a dental visit in the past 3-6 months, and indicated having a preventive appointment for their last dental visit. These findings were consistent with the literature, where veterans may have dental insurance benefits, but are more likely to self-report a status of fair or poor. In this study, perceived oral health status had a statistically significant impact on lack of dental home, having a dental visit within the past six months, financial barriers to dental care, and experiencing a toothache over the last 12 months (Table III).
The cost of oral healthcare was frequently reported as a challenge, with more than half of the VADC ineligible respondents reporting cost as a barrier to accessing any type of oral healthcare. Co-pays and out-of-pocket expenses appear to be barriers for even for those with dental benefits, consistent with the limited literature available on this population. Of the VADC ineligible respondents in this study who indicated that they had dental benefits from sources outside the VA, 20% indicated they had TriCare Retiree Dental Plan, administered by Delta Dental. The TriCare plan has significant limitations for non-preventive procedures, requiring one year of enrollment prior to covering major work (crown and prosthesis), and only pays a percentage of allowable amount determined by the plan, resulting in significant out-of-pocket costs.36
Nearly one-third of VADC ineligible respondents reported having Medicaid or Medicare as dental insurance. While Medicare Advantage plans may offer limited dental benefits, it is important to note that the VA does not partner with Medicaid or regular Medicare. This lack of partnership further complicates access to care for non-service related healthcare needs, particularly if these services are provided through the VA. Furthermore, it is generally recognized by the dental community that most private practices do not partner with Medicaid or Medicare dental plans for adult patients due to low reimbursement rates.
Limitations to this study include the potential bias of a self-reporting survey. In addition, the survey questions did not address whether participants had applied to the VA for healthcare benefits, the qualification criteria of veterans who qualified for VADC, or if existing dental insurance benefits were provided by a spouse or parent. Cultural factors that could be impacting veterans' access to care were not addressed in the survey and the convenience sample limited the generalizability of the results. Future research could address these limitations.
Conclusion
Results from this study show that veterans value the importance of oral health. However, strict VADC regulations and cost of care, are the greatest barriers to accessing oral healthcare services for individuals who are ineligible for dental benefits. Further research is needed to impact Veterans Administration policies and decrease oral health disparities in the growing veteran population.
Footnotes
Valerie Nieto, RDH, BSDH, is a 2019 graduate dental hygiene candidate of the Department of Periodontics and Oral Medicine, University of Michigan School of Dentistry, Ann Arbor, MI. Michelle Arnett, RDH, MS, is a clinical assistant professor, Department of Primary Dental Care Division of Dental Hygiene, University of Minnesota School of Dentistry, Minneapolis, MN.
Danielle Furgeson, RDH, MS, DHSc is a clinical assistant professor and Director of the Graduate Dental Hygiene Program, Department of Periodontics and Oral Medicine, University of Michigan School of Dentistry, Ann Arbor, MI.
Valerie Nieto was the 2018 recipient of the undergraduate ADHA/Sigma Phi Alpha Journalism Award sponsored by:

This manuscript supports the NDHRA priority area Population level: Access to care (vulnerable populations).

- Received August 10, 2018.
- Accepted March 14, 2019.
- Copyright © 2019 The American Dental Hygienists’ Association





{kind=link}
{kind=link}
{kind=link}